
A Draft for an Integral Concept of Dementia
Translation of my Masterthesis in Gerontology (M.Sc.) at the University of Erlangen, 2011
"Entwurf für ein integrales Demenz-Konzept"
Note: Most of the text was translated with Deepl Pro and proofread afterwards. I have read Wilber in German, I apologize for imprecise translations of certain
integral terms into English. All German citations are translated with deepl.com from the original if not mentioned otherwise. The English citations should now be all original. Please note also,
that this is a corected version of the master thesis in that sense, that I corrected or adjusted all quotations with errors, which I have to confess that I have found some in the original, when I
was looking up the original English citations.
Table of content
1 Introduction
2 State of research on definitions and concepts of dementia
2.1 Definitions: What is dementia?
2.2 Concepts and models of dementia
2.3 Summary
3.1 The Integral Theory according to Wilber
3.1. Fundamental principals of Integral Theory
3.1.1 The quadrant model
3.1.2 Lines of development
3.1.3 Levels of development
3.1.4 Types
3.1.5 States
3.1.6 Summary of the structural elements of Integral Theory
3.2 Integral Methodological Pluralism
3.2.1 Validity claims
3.2.2 Methodological pluralism: quadrants and zones
3.2.2.1 Methodologies of the inner-individual dimension
3.2.2.2 Methodologies of the inner-collective dimension
3.2.2.3 Methodologies of the exterior-individual dimension
3.2.2.4 Methodologies of the exterior-collective dimension
3.2.3 The three strands of knowledge
3.3 Summary: Integral research
4 Key assumptions for an integral dementia concept
4.1 Holon dementia
4.2 Focus of this thesis
4.3 Terminology
4.4 Epistemological research framework
4.4.1 Procedure for the development of an integral dementia concept
4.4.2 Procedure for reviewing an integral dementia concept
1 Introduction
The medical perception of dementia as a disease or disorder is still prevalent, not only in the medical literature (Förstl, 2009a; Mahlberg & Gutzmann, 2009a), but also in politics (BMFSFJ, n.d.) and advocacy groups (Deutsche Alzheimer Gesellschaft, 2008). Public opinion is also influenced by this view, as the media frequently show a medically dominated understanding of dementia, as it can be seen from ramble through the online portals of well-known magazines such as Stern or Spiegel or even daily newspapers from the Frankfurter Allgemeine Zeitung to Bild. Television magazines also do not dispense with 'medical expertise' when they have dementia as a topic (Quarks & Co, 2010).
But there are also new approaches to dementia, such as by Peter Whitehouse (Whitehouse & George, 2009), who, as a former authoritative scientist in pharmacological dementia research, 'debunks' the myth of Alzheimer's and contrasts his model of brain aging with the medical concept of dementia as a disease. Richard Taylor, a person affected by dementia, has also contributed to changing the image of dementia with his autobiographical publication Alzheimer's and I, and his provocative thesis therein "There is no such thing as Alzheimer's disease!" (Taylor, 2008, 36).
In Germany, two congresses resp. conferences on dementia in 2010 have shown that the image of 'dementia' is currently in a process of change. At the Dementia Fair Congress in April 2010 in Nuremberg, Helga Rohra, member of the board of the Alzheimer Society Munich and a person with dementia, was still accused of lying by a medical doctor during her presentation about her experiences with the diagnosis and the way into the public eye, because in his opinion she could not be affected by dementia due to her ability to articulate. At the open conference of the German Ethics Council on the topic of Dementia - End of Self-Determination? in Hamburg in November 2010, Helga Rohra could again be seen taking part in the concluding panel discussion with representatives from science and politics as a partner in conversation as a matter of course (Deutscher Ethikrat, 2010). If one takes these two events together from the perspective of the congress and conference visitor, then within a few months a change took place in the acceptance of Mrs. Rohra as a 'competent person' from a person affected by dementia who was not accepted by the scientific community to an interlocutor who was included as a matter of course by the scientific community.
The image of dementia seems to be in a gradual change, at least according to the facts reported here. But one question remains unanswered: What is dementia? For even if public and scientific attention is slowly opening up to a changed picture of dementia, the medical supremacy of definition does not seem to have changed much yet, as Wetzstein (2005a), Whitehouse and George (2009), and Wißmann and Gronemeyer (2008) show. Can dementia continue to be defined as a disorder when affected persons and scientists discuss it at the same table?
The above examples are meant to be representative of a variety of perspectives, opinions, and sometimes controversial viewpoints in the current discussion of the question: what is dementia? So far, there is no model, no theory, no concept that can provide an answer that all individuals and groups involved can agree upon. There is also no model that is comprehensive enough in its scope to combine the different scientific findings and professional as well as personal positions and to bring them together in one explanatory approach.
Integral Theory according to Ken Wilber (1997, 2000a) claims to be all of these: comprehensive, unifying, and bringing together seemingly conflicting positions. As a theory of consciousness that builds on the work of numerous theorists in philosophy and consciousness research (McIntosh, 2007; Wilber, 2000), and which is shown to be a multidimensional model in its structure (Wilber, 1997), it lends itself as a theoretical basis for bringing together the various concepts, models, and opinions on dementia with the goal of an overarching, comprehensive concept of dementia that does not seem to exist in this form to date.
This thesis pursues the epistemological claim to develop a draft for an integral dementia concept based on Integral Theory, with which the phenomenon of dementia can be represented in its manifold relations in such a way that as many as possible of the hitherto seemingly contrary positions on dementia can be included. It will be examined to what extent a synthesis of dementia and Integral Theory can be realized and meaningful, and to what extent Integral Theory is suitable to represent the phenomenon of dementia in the most comprehensive way possible.
Chapter 2 provides an introduction to the current state of research on definitions and concepts of dementia under the question "What is dementia? Chapter 3 provides an introduction to Integral Theory, with a brief overview of its history, (scientific) reception, and theoretical background. An overview of the structural elements and the Integral Methodological Pluralism as a basis for the further procedure in this thesis will follow. Chapter 4 sets up the premises for the subsequent epistemological elaboration of the basic structures of an integral dementia concept by describing in detail the object of research, terminology, and approach. Chapter 5 examines whether it is possible to describe dementia in its multidimensionality with the help of Integral Theory as an epistemological guide and thus to develop a draft for an integral dementia concept. Chapter 6 reviews the results of the previous chapter by means of a literature analysis. The results are discussed in Chapter 7 with regard to the extent to which the Integral Theory appears suitable as a basis for a dementia concept. Furthermore, the theoretical approach of this work will be briefly reflected on and concluded with an outlook on possible further research.
Finally, two clarifications of terms are necessary:
The persons, who are in the center of the consideration of scientific research around dementia, are called in this work people with dementia (Wißmann & Gronemeyer, 2008) or "the person affected" or "affected person". [Unfortunately, there is no appropriate English translation for the German word "Betroffener".] The term affected person originates from the field of social work and refers to people who usually find the occasion that makes them an affected person unpleasant (de:Wikipedia, Betroffene). Nevertheless, the use of the term remains imprecise, because also the relatives of people with dementia often perceive their situation as unpleasant (Engel, 2008) and are therefore 'affected'. For this reason, a more precise definition is necessary: In this paper, the term affected is used exclusively for the group of people with dementia.
Another preliminary remark seems necessary for the use of Wikipedia: In this work Wikipedia is used as an encyclopedic source of information. In science, there are reservations about the scientific relevance and quality of Wikipedia articles (cf. among others Nentwich, 2009; König, 2009), so the point of view and procedure for dealing with Wikipedia sources will be briefly explained here.
Wikipedia is defined as an encyclopedic project via its own guidelines (de:Wikipedia, Wikipedia). It is thus not scientific literature, but as an encyclopedia it reflects the state of scientific positions. Numerous scientists and scholars contribute to Wikipedia articles, and the quality of the articles is high in many areas (König, 2009). However, the articles can also have obvious or subtle quality deficiencies (König, 2009; Weber, 2005), so a personal quality check of the articles is advised before using them in a scientific context.
In this work, articles of the German or English Wikipedia are consulted, which are characterized by a professional discussion of the content (on the discussion culture as a quality feature, see Haber in Staas, 2010) as well as do not contain any quality assurance entries at the time of the call (see de:Wikipedia, Enzyklopädie/Qualitätssicherung in der Wikipedia). Furthermore, Wikipedia articles are predominantly used to define terms and to present a current state of discussion.
Since there are no clear guidelines for the citation of Wikipedia, the following procedure is chosen: The complete article name without year is given after 'Wikipedia', in the list of sources after 'Wikipedia. Artikelame' the date of the used article version is mentioned. In this way, the information content used can be traced on the basis of the version history of an article, also after long periods of time.
2 State of research on definitions and concepts of dementia
Many textbooks on dementia start with the basic medical facts about the development and course of a so-called dementia-related disease, which are accepted as valid by a large part of the scientific community (e.g., Förstl, 2009a; Mahlberg & Gutzmann, 2009a). Data on prevalence and incidence open up various professional articles on dementia, e.g. on prevention (Laske, 2007), nursing care concepts (Nocon, Roll & Schwarzbach et al., 2010) or on exercise programs for people with dementia (ProAlter, 2011). Information about forms of dementia, about current and future costs of care for people with dementia, about risk potentials and prevention possibilities can be found regularly in many media; searches on the online portals of Spiegel, Stern and Focus, but also of Bild [some popular German magazines and newspapers], yield a high number of articles on dementia. All sources have in common that details are reported extensively, but rarely the question is answered: What is dementia actually, what is this phenomenon that has broken into the health care system, the media and above all into the everyday life of so many people in such a dominant way? This chapter provides a brief overview of current answers to this question.
The primary interest of this thesis is not the much-cited details. Rather, it is an attempt to gain an overview of dementia in its entirety. It will be attempted to describe and capture dementia in as many facets of its appearance as possible. This also includes details such as epidemiology, symptomatology and therapy, but they are ultimately only of minor interest with regard to a comprehensive overall picture of dementia in its possibly much broader references up to legal sciences, literary research, urban planning and architectural aspects and much more. Therefore, for the time being, reference is made to the relevant literature for the general data on dementia (Förstl, 2009a; Kastner & Löbach, 2007; Kieckebusch, 2010; Mahlberg & Gutzmann, 2009a). Where necessary in the context of this thesis, the relevant data will be referred to later.
The question "What is dementia?" cannot be answered with a simple, universally valid formulation. Nevertheless, it is a question that concerns almost all persons involved in the phenomenon of dementia: What is dementia? How can this phenomenon be described, explained, researched and perhaps even eliminated? What is it? A disease? Or is it rather a normal phenomenon of old age (Plemper, 2010; Whitehouse & George, 2009)? In recent years, more and more voices have been raised calling attention to the increasing demonization of the alleged disease dementia and the one-sided occupation of the interpretive authority over this phenomenon by the medical experts (Dammann & Gronemeyer, 2009; Wetzstein, 2005a; Whitehouse & George, 2009; Wißmann & Gronemeyer, 2008).
The current state of research on the aforementioned questions is approached from two directions in the following: First, the current state of definitions of dementia is considered in order to gain an overview of how the question "What is dementia?" is answered in current scientific, practice-based, and general discussions, and which streams and fields of science provide these answers. Second, the research landscape is reviewed for theories, models, and concepts of dementia that encompass multiple aspects of dementia, if possible, to gain an orientation to the current state of research on dementia in its entirety.
Introductory it must be pointed out that in the context of this work dementia is not differentiated into different forms. For this work, the phenomenon of dementia itself, in all its facets and references, is the guiding principle, not primarily differentiated according to specific symptoms, etiologies and therapies.
2.1 Definitions: What is dementia?
The challenge of answering the leading question of this chapter already starts with the terminology: dementia, with its original meaning "without mind" transferred from the Latin word dementia (Wißmann & Gronemeyer, 2008, 52), is a terminology that is not easy to describe in terms of content and, moreover, is mostly used synonymously with Alzheimer's disease by many people (Engel, 2011). An abstract definition of dementia does not seem to exist so far; the definition of the term is either emotionally determined by terms such as "disease of the century," "farewell to the ego," and the like (Wetzstein, 2005a, 11), or is often made via the diagnostic criteria of the leading medical science, as stated by Wetzstein (2005a) in her study on the ethics of Alzheimer's disease.
Definitions of dementia with the broadest possible validity are to be expected in various places in literature and other media: In the basic literature on dementia, by advocacy groups, by research institutions and health policy organizations.
The definitions of the World Health Organization (WHO) in the International Classification of Diseases (ICD-10) (DIMDI, 2010) and the American Psychiatric Association (APA) in the Diagnostic and Statistic Manual (DSM-IV) (Saß, Wittchen, Zaudig & Houben, 2003) can currently be regarded as the most authoritative guiding definitions. Wetzstein (2005a, 42) speaks of a certain monopoly position of both institutions in the classification of diseases. According to Wißmann & Gronemeyer (2008), these classification systems reflect "what is the basis for medical thinking and action" (Wißmann & Gronemeyer, 2008, 33). Thus, it can be assumed that they can also be regarded as guiding definitional instances for dementia research.
ICD 10: Dementia (F00-F03) is a syndrome due to disease of the brain, usually of a chronic or progressive nature, in which there is disturbance of multiple higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgement. https://icd.who.int/browse10/2016/en#!/F00-F09
DSM-IV: The main feature of dementia is the development of multiple cognitive deficits, with memory impairment and at least one of the following cognitive impairments: Aphasia, Apraxia, Agnosia, or Executive Function Impairment. [...] (Saß, Wittchen, Zaudig & Houben, 2003)
Although there are differences (Wetzstein, 2005a; Wißmann & Gronemeyer, 2008), which are not reflected in the excerpts of the definitions presented here, both institutions answer the question "What is dementia?" with a description of dementia as a syndrome whose leading symptoms are cognitive disorders (Wißmann & Gronemeyer, 2008).
On the website of the Deutsche Alzheimer Initiative (2008), which can be regarded as the overarching advocacy group for people with dementia and their relatives in Germany, a definition of dementia can be found after the search steps 'Alzheimer's disease/dementia' and 'Frequently asked questions and answers':
Dementia is one of the most common health problems in older age. The term "dementia" comes from Latin and literally means "away from mind" or also "without mind". It is understood to mean disorders of mental-emotional performance occurring in different compositions, such as memory disorders and thinking difficulties with a clear awareness, speech disorders, changes in mood control and social behaviors, making it very difficult to cope with everyday life. Dementia can have many causes, with Alzheimer's disease [...] being the most common [...]. ("Deutsche Alzheimer Gesellschaft," 2008)
Also here the focus is on memory disorders, which according to this understanding are caused by Alzheimer's disease (and other diseases). Thus, a causality is named here: First the Alzheimer's disease appears, by which then the disturbances are caused.
The dementia guide of the Ministry for Family Affairs, Senior Citizens, Women and Youth (Bundesministerium für Familie, Senioren, Frauen und Jugend, BMFSFJ) (n.d.) provides an explanation of the term in the section 'Medical background'/'Dementia'.
Dementia is a umbrella term for more than 50 forms of the disease. They progress differently, but all lead to long-term loss of mental capacity. The causes of dementia are manifold. A basic
distinction must be made between primary and secondary dementias. Secondary dementia is the result of another, already existing underlying disease. (BMFSJF, n.d.)
In this context, the answer to the question "What is dementia?" is a purely medically based statement that is reduced to naming the various clinical pictures. Clearly, dementia is named as a disease.
The Dementia Competence Network [Kompetenznetz Demenzen] (n.d.), as a research association of mainly psychiatric clinics, also aims in its definition of dementia at the concept of disease. The following definition on the website of the Competence Network is primarily intended for people with dementia and their supporters. For the specialized public no own definition is given but referred to numerous guidelines.
Dementias are diseases that lead to the loss of mental and physical abilities, so that the affected persons in advanced stages can no longer lead an independent life. (Dementia Competence Network, n.d.)
Demenz Support Stuttgart (2010a) does not provide a literal definition of dementia on its website. The closest possible approximation to a form of definition that can be found there is part of the philosophy of the institution, which sees itself as a "mediator and moderator between the highly diverse groups of actors, professions, disciplines and perspectives involved in addressing the societal challenge of dementia" (Demenz Support Stuttgart, 2010a). A medical definition or a definition of a disorder is searched for without success.
Dementia confronts us with crucial social and cultural challenges. Real improvements will only be achieved if we say goodbye to ingrained patterns of perception and prevailing attitudes. (Dementia Support Stuttgart, 2010a)
A definition of what dementia is, can also not be found on the website of Aktion Demenz e.V. (n.d.a). However, an answer to the question "What is dementia?" becomes clear in the Esslingen Appeal of the initiative (Aktion Demenz, n.d. b), but focuses on the people with dementia, not dementia itself:
People with dementia are citizens! [...]
People with dementia do belong! [...]
People with dementia have rights! [...]
People with dementia concern us all! [...]
People with dementia need our fantasy! [...]
(Aktion Demenz, n.d. b)
Here, a citizenship or civil society understanding of dementia becomes obvious.
The comment by Wetzstein (2006), who, as a representative of an ethical perspective on dementia, criticizes the absolutization of the medical perspective on the overall debate, appears as a summary of these definitions and positions on dementia: "However, a biomedical concept of dementia, which was absolutely appropriate for medicine, now found its way into the social discourse on dementia, to a certain extent via a supposed scientific objectivity." (Wetzstein, 2006, 39). In the definitions and viewpoints on dementia presented here, the dominance of this biomedical concept becomes visible. Many institutions involved in the topic refer to a disease concept as a characteristic of dementia and focus especially on memory impairment. Nevertheless, with Demenz Support Stuttgart and Aktion Demenz, two institutions clearly differ from this concept, so that it is no longer possible to speak of a general dominance of the discussion by the medical definition, even if this clearly predominates in the selection of definitions presented here.
A brief overview of some definitions and explanations of terms in foundational literature on gerontology and dementia will clarify the extent to which the picture that has emerged so far of a medically dominated definition oriented toward disease or disorder is also represented in this field, or whether a different picture is emerging.
In their Introduction to Gerontology [Einführung in die Gerontologie], Wahl and Heyl (2004) see dementia as a disease. Förstl (2009a), in the basic work Dementias in Theory and Practice [Demenzen in Theorie und Praxis], refers to the ICD-10 when answering the question What is dementia? and describes the dementia syndrome as "a secondary deterioration of a previously greater mental capacity" (Förstl 2009b, 4). Mahlberg and Gutzmann (2009b) also refer to dementia disorders in Recognizing, Treating, and Caring for Dementia [Demenzerkrankungen erkennen, behandeln und versorgen]. Kieckebusch (2010) differentiates in her Psychological Dementia Diagnosis [Psychologische Demenzdiagnostik] that dementia is "in the narrower sense not a disease, but rather an increasing impairment of mental performance or a brain-organic pathological degradation" (Kieckebusch, 2010, 17). The S3 Guideline Dementias, in the development of which the Deutsche Alzheimer Gesellschaft was also involved, formulates: "Dementias are defined by the degradation and loss of cognitive functions and everyday skills." (DGPPN & DGN, 2009, 11). Thus, the basic literature cited here is relatively clearly oriented to a disease or disorder concept.
Finally, a look at the perspective of those affected gives a little insight into the fact that a medically dominated picture is not helpful or sufficient for all people involved in the phenomenon of dementia. People with dementia are also first confronted with the classical definitions of dementia. For example, Taylor (2008), an American psychologist affected early by dementia, says dementia is "a pattern of symptoms suggestive of one disease or a combination of several diseases" (Taylor, 2008, 36), but formulates a little later, "From my point of view, from that of a person living with this diagnosis [Alzheimer's disease, B.W.], far too much importance is given to the label, the name, and the symptoms that usually accompany the condition, whereas too little importance is given to the people who have the disease." (Taylor, 2008, 42). From the internal perspective of dementia, the attempt to define it, as attempted here from a scientific perspective, is seemingly irrelevant, at least to some persons affected.
Summarizing, Wetzstein's (2005a) research findings in which she states a lack of abstract definitions still seem to be relevant, as does the dominance of a medical model she notes. "Anyone who follows the public debate about Alzheimer's disease in the media is struck by the following: Alzheimer's disease appears as a purely medical problem for which physicians alone are considered competent." (Wetzstein, 2005a, 38). In many cases, dementia seems to be nothing more than a disorder, a disease. Other aspects, such as the civic approach represented by Demenz Support Stuttgart and Aktion Demenz, are only slowly coming into the focus of (scientific) debate.
Therefore, in the following, the state of research on dementia concepts as further explanatory models will be considered in more detail.
2.2 Concepts and models of dementia
Beyond the mere definition of dementia as presented in the previous paragraph, there are many detailed explanations for dementia. Following Wetzstein (2005a), the term "dementia concept" will be used for these in the following. In Wetzstein's study on an "Ethics of Dementia" [Ethik der Demenz] (2005a), the state of research on concepts of dementia was presented, so that this work can build on these results. As already shown in the previous section, Wetzstein's findings on the definition of dementia have changed little since 2005.
Wetzstein (2005a) explores the term dementia concept in detail. So she identifies, among others, dementia concepts of the constructivist tradition, which she rejects because no moral differentiation of different positions is possible (Wetzstein, 2005a, 15). Furthermore, she identifies concepts by and in the tradition of Tom Kitwood, which she likewise rejects as moderately constructivist, among other things because the model opposed to the medical model does not appear to be feasible (Wetzstein, 2005a, 15). More recent approaches by Post and Whitehouse, to which she attests a similar (i.e., ethically oriented) goal as her own concept, are, however, subject to the shortcoming, in Wetzstein's view, "that they do not take the trouble to systematically elaborate criteria of the current dementia concept" (Wetzstein, 2005a, 15). According to her research, a purely medical concept of dementia dominates, even though she acknowledges at a later point that there are also approaches in medicine to open to insights from, for example, social psychology (Wetzstein, 2005a).
It [Wetzstein's study, B.W.] is based on the hypothesis that the Alzheimer's disease problem complex is
currently based on a dementia concept determined by scientific criteria. This current dementia concept is first of all based on medical statements about dementia and has implications and
consequences from here. Since medicine, in pursuing its own mission of diagnosing disease and curing or alleviating suffering, never acts on phenomena without presuppositions, the current
dementia concept is necessarily based on limitations. If this supposedly comprehensive concept is transferred to the public, the phenomenon of Alzheimer's disease experiences a significant
reduction. (Wetzstein, 2005a, 16).
Wetzstein is not the only one with this criticism of the medically dominated dementia concept. Wißmann and Gronemeyer (2008) also call for a critical discussion of ICD-10 and DSM-IV and formulate as a goal "a broadly conducted debate about a new and holistic dementia definition, which would have to be the basis of all social groups, not the only one of medicine" (Wißmann & Gronemeyer, 2008, 33). Dammann and Gronemeyer (2009) justify their criticism of medicine and the billion-dollar business with dementia as follows:
Until today, no clear biological-organic causes could be identified in the majority of people suffering from "brain disorders", so that most dementia diagnoses are in fact interpretations, i.e., nothing but the interpretation of symptoms. (Dammann & Gronemeyer, 2009, 12)
Finally, Whitehouse and George (2009) 'debunk' the myth of Alzheimer's, take an unequivocal stand against the interpretive sovereignty of medicine in matters of dementia, and advocate a modified concept of dementia, which in their case consists of accepting the changes defined by medicine as dementia as part of normal brain aging and adjusting one's life accordingly (Whitehouse & George, 2009).
Looking at the alternative concepts and models proposed, the respective authors turn away from the medical definitional sovereignty in their concept development, but contrast the previous model with new concepts, which are often also entrenched in a perspective stance, such as Wißmann and Gronemeyer (2008) with their civil society approach, and Whitehouse and George (2009) with their brain aging approach.
However, what all recent concepts have in common (Wetzstein, 2005a; Whitehouse & George, 2009; Wißmann & Gronemeyer, 2008) is that they call for a holistic, integrative approach and want to see other relevant sciences included.
Dementia cannot be the concern of a single or a few disciplines. Dementia concerns everyone! Ethics, medicine, culture, philosophy, education, sociology, nursing, theology, psychology and anthropology: they all have an equal contribution to make to the discourse. Scientists, politicians and care practitioners, family caregivers, civic activists, people with dementia, young and old: they all have a voice. (Wißmann & Gronemeyer 2008, 76)
Both the approaches of Wetzstein (2005a) with a theological-ethical orientation and Wißmann and Gronemeyer (2008) with their civil society model are important approaches on the way to a comprehensive dementia concept. However, they leave out aspects that are equally important components of the phenomenon of dementia, such as economic or macroeconomic issues (Kiencke, Rychlik, Grimm & Daniel, 2010), the question of the spatial-architectural integration of dementia (Marquardt, 2006) or the literary processing of the phenomenon (Schnell & Mitzkat, 2006). The concepts considered in depth here (Wetzstein, 2005a; Whitehouse & George, 2009; Wißmann & Gronemeyer, 2008) are thus comprehensive in their perspective orientation, but not far-reaching enough to give space to as many aspects of the phenomenon of dementia as possible or to offer points of connection also for marginal topics. It should be noted, however, that none of the concepts mentioned makes this claim for itself.
2.3 Summary
Based on the findings of several studies, in this chapter it could be shown that in the current professional as well as general discussion a medically dominated picture prevails, which however - this could also be shown to some extent - is not sufficient to meet and correspond to the concerns of all participants and the challenge of dementia on all levels. In the definitions of some important institutions in the context of dementia, a dominance of a medical disease concept of dementia could be found. Both in these and especially in the basic guidelines (ICD-10, DSM-IV, S3 Guideline on Dementias [S3-Leitlinie Demenz]), terms such as disorders, disease and reduction dominate (cf. ch. 2.1). The same applies to the professional literature (cf. section 2.1). Newer approaches of concepts, which want to abolish the dominance of medicine, are available, but remain connected to a perspective view (cf. ch. 2.2).
In the following chapter, Integral Theory will be presented as a theoretical model that claims to be so comprehensive that it can largely integrate or link all aspects of an issue.
3 The Integral Theory according to Wilber
In the above outlined state of research, it became clear that conventional dementia concepts are dominated by a medical understanding of dementia. Various areas seem to have been left out so far, or have only been poorly covered by scientific research, as scientists, people with dementia and advocacy groups increasingly complain (Taylor, 2008; Wetzstein, 2005a; Whitehouse & George, 2009; Wißmann & Gronemeyer, 2008).
The goal of this paper is to develop a blueprint for a dementia concept that can integrate as many perspectives as possible. In order to take into account the different perspectives of people with dementia, relatives and scientists of different disciplines, treating physicians, caregivers, but also other stakeholders, a multidimensional framework is needed that allows and includes many perspectives on an equal footing.
The Integral Theory according to Ken Wilber (2001a, 2006a) claims for itself a multidimensionality that makes it possible to include previously competing views and concepts of scientific research, practical activity as well as individual experiences in an explanatory model.
The word integral means comprehensive, inclusive, non-marginalizing, embracing. Integral approaches to any field attempt to be exactly that: to include as many perspectives, styles, and methodologies as possible within a coherent view of the topic. In a certain sense, integral approaches are "meta-paradigms," or ways oto draw together an already existing number of separate paradigms into an interrelated network of approaches that are mutually enriching. (Wilber, quoted in Esbjörn-Hargens, 2009, 1)
Integral Theory is a rapidly growing current within the large field of integral studies since the early 1980s, building on the work of American philosopher Ken Wilber (for the distinction between integral theory and integral studies, see Esbjörns-Hargens, 2009). Drawing on the work of preceding integral theorists, such as Teilhardt de Chardin and Jean Gebser (McIntosh, 2007), Wilber developed his integral explanatory model for phenomena of consciousness in numerous publications (including Wilber, 1997, 2000, 2001a, 2006a). The model is also known as the integral approach, quadrant model, or AQAL (all quadrants, all levels), and is increasingly used in various professions and scientific fields (Esbjörn-Hargens, 2009; Integral Research Center, 2009). In recent years, Integral Theory has also been increasingly received in German research (Fuhr & Gremmler-Fuhr, 2004; Weinreich, 2005; Küpers, 2006; Wittrock, 2008).
Even though Integral Theory is understood as a theory by many theorists and users, it should be noted that it is often referred to as a worldview (Wikipedia, Integral Theory), and is subject to numerous criticisms in terms of scientificity (for this, see, among others, the discussion pages of the German and English Wikipedia articles on Integral Theory; de:Wikipedia, Diskussion:Integrale Theorie; en:Wikipedia, Integral Theory; en:Wikipedia, Talk:Integral Theory). For a more in-depth discussion of the critics of Integral Theory, I refer to McFarlane (2000), McIntosh (2007), and Meyerhoff (2006) as examples.
Despite these criticisms, this thesis connects to the increasing acceptance and application of Integral Theory in the German and international scientific community (see references above). By applying the theory as an epistemological model, it aims to contribute to a broader view of dementia, not to a fundamental discussion of Wilber's Integral Theory.
In this work, Integral Theory is intended to serve as an epistemological guideline for the theoretical elaboration of a dementia concept that provides a framework for bringing together the various currents and explanatory models surrounding the phenomenon of dementia. In order to present the theory in its claim of a comprehensive approach (Wilber, 2006a) as a framework for an integral dementia concept, it will first be described in its basic elements without already making references to the subject area of dementia. While chapter 3.1 presents the basics of Integral Theory, chapter 3.2 will present the possibilities of its scientific application. Chapter 3.3 gives a summary of Integral Theory with regard to an integral research process.
3.1 Fundamental Principles of Integral Theory
A basic assumption of the Integral Theory is the evolutionary principle as the basis of all phenomena that have developed since the Big Bang, which almost all sciences agree to be the starting point of all being on earth (Wittrock, 2008).
Evolution is a wildly self-transcendence process: it has the utterly amazing capacity to go beyond what went before. So evolution is in part a process of transcendence, what incorporates what
went before and then adds incredibly novel components. The drive to self-transcendence is thus built into the very fabric of the Kosmos itself. (Wilber, 1996, 23)
Furthermore, it is assumed that evolution always moves in the direction of increasing complexity with increasing differentiation and increasing structuring, whereby the newly emerging higher levels always include and transcend the lower levels (Wilber, 2000a).
The concept of the holon is another basic assumption of Integral Theory (Wilber, 2000a). It states that in both biological and social contexts there are no entities that are completely independent of each other, whereby entity can be understood as a collective term for everything that is, or also as the "unspecified existence of something" (de:Wikipedia, Entität). The individual forms of existence are always embedded as individual parts in a whole and at the same time consist as a whole of different parts, which in turn are each independent wholes (and parts). "Each of these entities is neither a whole nor a part, but a whole/part, a holon." (Wilber, 1996, 20). Each holon stands in a hierarchical relationship to its higher level (from which it is included and transcended) and to its lower level (whose various parts it includes and transcends). This hierarchy of wholes that are part of another whole (de:Wikipedia, Holon) is also called holarchy. Development, according to this understanding, occurs through inclusion and transcendence of what has gone before (Wilber, 1997). All higher evolved entities (such as humans) have emerged from continuous transcendence of 'lower' entities (atoms, cells) without ceasing to exist, but being included in the higher evolved form.
From the findings about holons and holarchies came the further conclusion that all holons appear in four dimensions. All holons have an individual and a collective manifestation. "For example,
where there is individual consciousness, there is a collective culture to which that individual belongs. And as the consciousness of the individuals within a culture evolves, so does the culture
as a whole." (McIntosh, 2007, 220). Each holon further has an inner dimension and an outer dimension that are always evolving in interdependence. "Wilber also recognized that as the complexity of
a biological organism's exterior form increases, there is a corresponding increase in the complexity of that organism's consciousness." (McIntosh, 2007, 219). In short, there is always an inside
and an outside, a singular and a plural. Intertwined with each other, they represent four dimensions of reality, "at least four irreducible perspectives (subjective, intersubjective, objective,
and interobjective) that must be consulted when attempting to fully understand any
issue or aspect of reality." (Esbjörn-Hargens, 2009, 2). The multi-perspectivity of reality is consequently another basic integral assumption, whereby it is assumed that every occurrence
continuously unfolds in these four dimensions (Wilber, 2006a).
In summary, Integral Theory aims to bring together a wide variety of theories, methodologies, and strands to an issue so that it can be viewed from multiple perspectives of equal importance. Originally based on insights from consciousness research and psychology (Wilber, 2000b), Integral Theory "weaves together the significant insights from all the major human disciplines of knowledge, including the natural and social sciences as well as the arts and humanities" (Esbjörn-Hargens, 2009, 1). For this purpose, it makes use of so-called structural elements that differentiate and clarify the development of holons or entities of consciousness in different fields and at different levels. According to the understanding of the Integral Theory, development takes place in the four areas already identified in the context of the holons, which are called quadrants. In each of these, developmental processes occur in different characteristics over different developmental phases (Weinreich, 2007, 2). Integral terminology uses the term lines for these properties and calls the phases levels. The recognition that development in certain areas often proceeds according to certain patterns (types), and temporally limited, changing states in or around the entity influence what happens, completes the integral understanding of development. Thus, five structural elements (quadrants, lines, levels, types, and states) emerge that together provide a model for describing the reality of a single phenomenon. They are presented in the following sections.
3.1.1 The quadrant model
With the quadrant model of Integral Theory (Fig. 1), Wilber has developed a graphical model that provides a well-understood framework for currently practiced integral thinking, research, and action. Despite some criticism (e.g., McFarlane, 2000), it is considered by many integral theorists to be the best current model for explaining the integral frame of reference (Esbjörns-Hargens, 2009). Criticism of the external-collective quadrant in particular is expressed by McIntosh (2007), but he himself says at the same point, "Despite its limitations, I think we can continue to use the quadrant model as long as we do not take it too literally." (McIntosh, 2007, 230). In this sense, the quadrant model and its structural elements, described in the following sections, should be understood here as an epistemological guide to a thinking and research process, not as a literal dogma to be followed.
The quadrant model (Fig. 1) visualizes that each fact or holon is differentiated into the four domains derived in the previous section, here called quadrants: The upper quadrants stand for the individual parts, the lower quadrants for the collective parts. The left quadrants stand for the internal, the right quadrants for the external aspects of a holon.
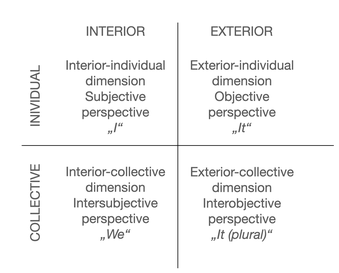
The upper left quadrant refers to the aspects of a holon from the inner-individual perspective. This area represents the inner processes accessible only to introspection, and is discussed in particular detail in most integral works. Phenomena such as "consciousness" (Wilber, 2001a,b) and "meditation" (Wilber, 2006a), which are intensively explored and practiced in the integral movement, are assigned to this quadrant. Here we are concerned with the subjective processes, with the 'I'.
In the upper right quadrant are found the aspects of a holon from the external-individual perspective. This is the area of observable behaviors and externally perceptible facts on the individual level, the area of objective aspects, the 'It'. This quadrant shows "what any individual event looks like from the outside." (Wilber, 2006a, 21).
The lower left quadrant is concerned with the internal perspective of collective phenomena. Here all cultural, commonly internalized aspects of a collective are considered; it is the realm of intersubjective understandings, the 'we'. "The Lower-Left quadrant is the study of shared interior meanings that constitute the worldview (or common worldspace) of collective or communal holons." (Wilber, 2000, 131).
The lower right quadrant gathers together all the external-collective aspects, the externally perceptible and measurable parts of a collective, a social system. It is the realm of the social environment, the 'they' (or also called 'it' plural). The individual is of interest here only insofar as it is part of a particular network or system whose functionality is central. "The Lower-Right quadrant, in other words, represents all the exterior forms of social systems, forms that also can be seen, forms that are empirical and behavioral [...]." (Wilber 2000, 128).
The quadrants thus illustrate that 'reality' appears in different dimensions, and that - if one wants to represent reality as comprehensively as possible - one has to approach it from many different perspectives. Each quadrant represents reality, but not the whole reality, but one aspect, one dimension of reality. In recent works Wilber (2006a) additionally distinguishes between quadrants (the perspective of a subject) and quadrivia (the perspective on an object) and puts forward the thesis that only for individual holons quadrants and quadrivia (i.e. the perspective of the subject and that on the object) are possible, but artifacts (for example a Coke bottle, cf. Wilber, 2006a) can only be viewed from a perspective on an object, i.e. they do not 'have' quadrants but only quadrivia (Wilber, 2006a). However, since the problem of artifacts is of only minor interest in the case of the present topic, further discussion of quadrivia will be left out here.
Similarly complex as the quadrivia, the Integral Theory becomes through the so-called zones, which are created by adding an external perspective to each quadrant. These eight zones, introduced in the recent work of Wilber (2006a), will be presented in more detail in chapter 3.2 within the framework of Integral Methodological Pluralism because of their relevance for scientific research.
At this point, the description of the structural elements of Integral Theory continues with the model of lines. It should be noted that in this work we deviate from the usual order of description in Integral Theory (first levels, then lines, cf. Esbjörn-Hargens, 2009; Wilber 2006a), as it seems to me to be the more sensible order for the later application to dementia as well as for the underlying understanding of development: development happens in different domains (lines) and extends within them over different levels.
3.1.2 Lines of development
The lines of development, also called streams (Wilber, 2001a), describe the phenomenon that development takes place in different areas within a quadrant. Individuals can reach different levels of development in different abilities, cultures are at different levels of development in different areas, states are differentiated differently in the individual areas of their organization.
Lines of development exist in all quadrants. "An integral practitioner can use lines as a diagnostic tool to ensure that these aspects are recognized and effectively addressed by individuals or groups." (Esbjörn-Hargens 2009, 9). The developmental lines of one quadrant correlate with those of other quadrants. Thus, neurophysiological changes in the external-individual realm cause changes in the line of consciousness in the internal-individual realm (and vice versa), which in turn affects lineages in the culture and system of the person concerned (Wilber, 2000). However, this does not mean that there is always uniform development in all domains and in all lines; on the contrary, development occurs to different degrees and at different speeds in different lines (Wilber, 2006a).
[...] some lines are necessary but not sufficient for others; some develop closely together. But on balance, many of the streams develop at their own rate, with their own dynamic, in their own way. A person can be at a relatively high level of development in some streams, medium in others, and low in still others. Overall development, in other words, can be quite uneven. (Wilber, 2001a, 44)
The upper left quadrant is the best documented area in the integral literature in terms of lines of development (Wilber, 2006a). The lines in other areas are rarely elaborated in detail by Wilber; however, the reception of Integral Theory by Esbjörn-Hargens (2009, 11) shows a differentiation of the other quadrants. The following figure 2 shows some exemplary lines in the respective quadrants.
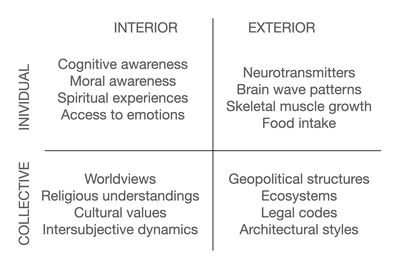
Within the individual lines, different phases of development can usually be described. These phases, called levels in Integral Theory, are explained in the following section.
3.1.3 Levels of development
Levels of development describe the phenomenon that development occurs continuously (albeit in different tempi) in the separate lines of the different quadrants. Growth or development proceeds in successively building levels (Fig. 3). Wilber (2001a) also speaks of waves of development, since a rather smooth transition from one level of development to the next is assumed. Occasionally, the term development stages is also used. However, since a developmental process rarely involves (or can be measured as) a clearly definable step up or down a level, the term levels or waves seems more appropriate, even though the level model shown in Figure 3 below suggests a stage-like progression of developmental levels.
The level model illustrated in Figure 3 using exemplary areas makes it clear that reality is a dynamic process, not a static persisting state. The levels represent the development of a holon over time, with the levels of the left quadrants representing the (increasing) depth of a development, and the levels of the right quadrants representing the (increasing) complexity of an issue (Esbjörn-Hargens, 2009).
Levels or waves in each quadrant demonstrate holarchy, which is a kind of hierarchy wherein each new level transcends the limits of the previous levels but includes the essential aspects of those same levels. Thus, each wave inherits the wave of the past and adds a new level of organization or capacity. (Esbjörn-Hargens, 2009, 8)
One of the best-known level models for the upper left quadrant that is drawn upon in the integral movement is Spiral Dynamics (Fig. 4), a developmental approach by Graves (Wilber, 2001a) that Beck and Cowan (2008) have extended. The model describes the development of value orientation using a spiraling upward model in which growth and development occurs as a smooth transition from one level to another (Beck & Cowan, 2008).
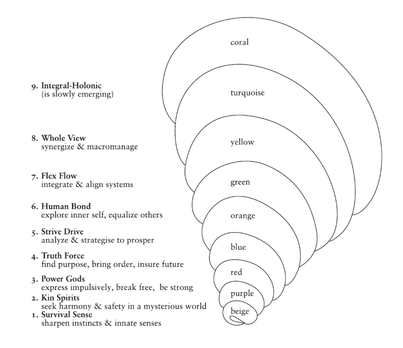
This model clarifies the understanding of levels, not stages, in which development occurs within a domain.
However, developmental processes not only differentiate into lines and levels, but further differentiate, as will be outlined in the following section, into specific typologies that can be of different types within each quadrant.
3.1.4 Types
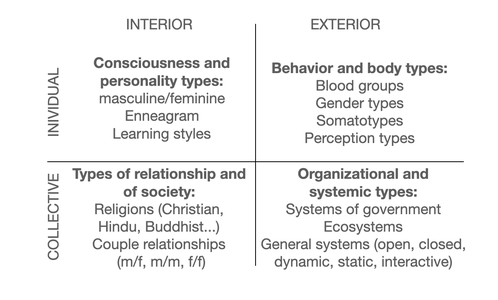
In all quadrants - and in all areas of development - one finds various typologies that must be taken into account when dealing in an integral way with an issue. Typologies show up within lines, levels and states. They mean nothing else than that within a domain two or more different kinds of development can take place, which are typical in a certain way, that is, can proceed in the same way in individuals, holons of the same kind and the same specific properties. "Typologies are, technically speaking, an expression of horizontal variance." (Habecker, 2010, 8). The simplest typology for the two upper quadrants is the distinction between male and female, i.e., gender types; another type model cited by Wilber (2001a) is the Enneagram, a personality typology of Sufi tradition that differentiates nine different types of cognitive-emotional behavior patterns (Palmer, 1991). However, typologies can also be found in all other quadrants (cf. Fig. 5), which illustrate that development in different individuals or collectives can proceed similarly in defined areas if certain identical initial conditions are present.
The consideration of the effects of a typology on the levels of a line of a quadrant, if necessary still with the addition of different states, assumes a degree of complexity, which is theoretically nameable, in the application in detail however probably only very laboriously convertible.
As the last structural element of the Integral Theory, the states follow in the next section as an element of temporally changing internal as well as external framework conditions for development processes.
3.1.5 States
The structural element of states, the final component of the Integral concept, is perhaps the most controversial element of Integral Theory in the scientific community, as exemplified by Belschner's (2010, 107) experience in the efforts to integrate Transpersonal Psychology into the scientific community. States can be identified in all four quadrants, as Figure 6 exemplifies.
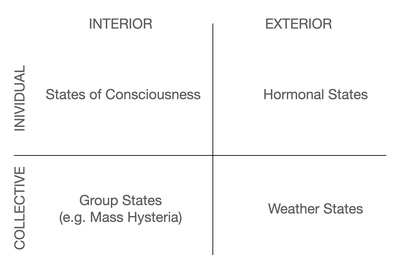
Esbjörn-Hargens (2009) describes the states-referring to all four quadrants-as "temporary occurrences of aspects of reality" (Esbjörn-Hargens, 2009, 13) and further remarks, "They also tend to be incompatible with each other." (ibid.). Waking state and deep sleep are excluding each other, likewise snowstorm and sunshine are usually mutually incompatible states; this is also true of many states in other quadrants.
In Wilber's writings, the various states of consciousness have their place primarily in the external-individual quadrant.
The inclusion of states is useful for practitioners because our realities both internally and externally are always shifting—all kinds of state changes occur throughout our day within ourselves and our environments. Including states allows us to understand many of the ways these shifts occur and why. (Esbjörn-Hargens, 2009, 13)
For the subjective quadrant, Integral Theory specifically refers to the natural states of consciousness: gross waking state, subtle dream states, causal formless states, state of the witness, and non-dual awareness (Wilber, 2006a). For the other quadrants, differentiated state models are hardly found in the integral literature.
3.1.6 Summary of the structural elements of Integral Theory
In the previous sections, the essential elements of Wilber's Integral Theory were presented. They form the basic framework by which a matter can be structured and the interconnections of its individual elements can be represented among each other. The way goes from a differentiation into four large areas of reality, the quadrants ( ch. 3.1.1) or also called dimensions, further to the different lines ( ch. 3.1.2) as the areas in which development takes place within each quadrant. Within these lines, development is a processual event that can usually be described in terms of different levels (ch. 3.1.2). Finally, these development processes differ again depending on the type (chap. 3.1.4) within which they take place and the states (chap. 3.1.5) to which they are subject.
The approach of Integral Methodological Pluralism (Wilber, 2006a), which will be explained in the following section, now points out the significance of these elements within scientific research and in which form they can be used.
3.2 Integral Methodological Pluralism
The approach of Integral Methodological Pluralism (IMP) (Wilber, 2006a; Wilber, 2006b; Wittrock, 2008) provides the framework to facilitate the application of Integral Theory and its structural elements presented in chapter 3.1 to concrete fields of work and epistemology. Against this background, Integral Theory is also useful in scientific research, as IMP makes the path of integral ways of knowing comprehensible and verifiable. There is no strict separation between the quadrant model and Integral Methodological Pluralism, as it might appear due to the structurally necessary subdivision of this work; rather, IMP is the extension and differentiation of the quadrant model.
Integral Methodological Pluralism (IMP) involves, among other things, at least 8 fundamental and apparently irreducible methodologies, injunctions, or paradigms for gaining reproducible knowledge (or verifiably repeatable experiences). The fundamental claim of AQAL Integral Theory is that any approach that leaves out any of these 8 paradigms is a less-than-adequate approach according to available and reliable human knowledge at this time. (Wilber, 2006a, 33).
Beyond the eight zones presented in section 3.2.2, the validity claims in section 3.2.1 can also be seen as a criterion for the responsibilities of different epistemological traditions as part of the IMP, as well as the approach to integral cognition described with the three strands in section 3.2.3. This section begins with the validity claims, as they can be seen as fundamental to the subsequent integration of the zones into the integral model.
3.2.1 Validity claims
From the structural elements outlined, integral research has the requirement to look at each issue from four interwoven perspectives. These four perspectives are represented by different schools, which so far have appeared as competitors rather than partners in science. As a representative, Wilber (1997) names scientific traditions and representatives of theoretical positions that have formulated their standpoint as representatives of 'truth' primarily also by distinguishing themselves from other methodologies and traditions.
Each approach is giving us, as it were, one corner of the Kosmos. Each is telling us something very important about various aspects of the known world. And none can be reduced to the others without aggressive and violent rupture, distortion, dismissal. (Wilber, 1997, 12)
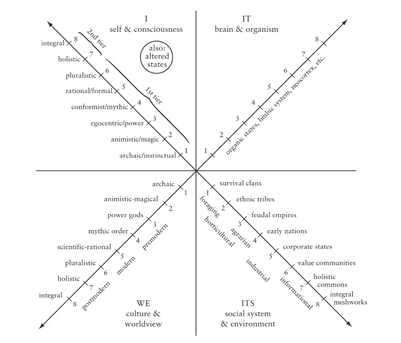
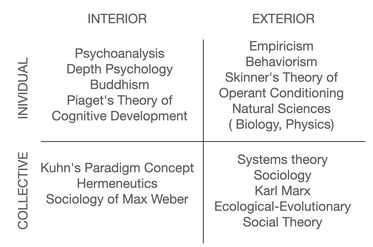
It is undisputed that all fields of science have produced important findings in their areas of responsibility (Wilber, 1997). Figure 7 provides an overview of some scientific and general epistemological traditions of the respective quadrants.
Criticized by the representatives of Integral Theory is that the different epistemological traditions claim to grasp truth for the whole without recognizing or admitting that their knowledge is 'true' but that this truth is only valid for a certain domain with certain injunctions and methodologies (what is also called quadrant absolutism in Integral Theory; Wilber, 2006a).
Wilber names interpretation and hermeneutics as representative methodological approaches for the two inner quadrants; he also calls science in these domains the 'broad sciences'. The methodological approaches representative of the two right quadrants are empiricism and positivism; these scientific tradtions are characterized as the 'narrow sciences' (Wilber, 2001a). All quadrants have different validity claims for epistemology, by which Wilber refers to Habermas' theory of validity claims (Wilber, 1997, cf. Fig. 8).
Each of these "four quadrants," in fact, has its own particular type of truth or type of "validity claim" — the ways in which it goes about accumulating and validating its data and its evidence. [...] And to say that none of these quadrants can be reduced to the others is to say that none of their respective truths can be dismissed or reduced, either. (Wilber, 1997, 12)
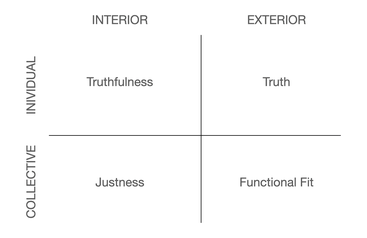
For the inner-individual quadrant, Wilber cites, among others, Freud, C.G. Jung, Jean Piaget, but also Aurobindo and Gautama Buddha as representatives of the ways of knowing of this quadrant (Wilber, 1997, 2001a). He calls it a "place of the 'inner' sciences" (Wilber, 2000, 161), whose most important epistemological traditions include psychoanalysis and phenomenology. The validity claim according to Habermas for an inner-individual researching science is subjective truthfulness. It is not a matter of obtaining objective data. Research in this quadrant makes use of subjective data obtained from the inner experience of individuals. "The validity claim here is not so much whether my statements match exterior facts, but whether I can truthfully report on my own inner status." (Wilber, 1997, 14).
Behaviorism, neurology, physics, and biology are mentioned as concrete epistemological traditions of the external-individual quadrant (Wilber, 1997).
Behavior can be seen, it is empirical — which is precisely why empirical science is always concerned only with the behavior of holons (the behavior of atoms, the behavior of gases, the behavior of fish, the behavior of humans) and wants nothing to do with nasty ol’ introspection, which involves, of course, the interiors of individuals. (Wilber, 2000, 128)
The validity claim of truth applies to this area of the empirical sciences. Wilber (1997, 52), following Habermas, speaks of a propositional truth that becomes 'true' by being consistent with an objective state of affairs. This validity claim not only holds in large areas of science, but also corresponds to most people's common understanding of truth in everyday life. What is true is what can be measured in some way according to defined criteria. "So common is propositional truth that it is often just called "truth" for short." (Wilber, 1997, 13). Thus, in integral terminology, when people speak of truth in their everyday life contexts, they are referring to the truth of the upper right quadrant - a truth that is based on measurable, objective data.
As in the inner-individual quadrant, the methodological approaches to the inner-collective quadrant are interpretive and hermeneutic; concrete scientific traditions are, for example, ethnology and ethics. The validity claim of this area is called justice. Sciences of this quadrant operate in the intersubjective space of trying to "understand how subjects fit together in acts of mutual understanding" (Wilber, 1997, 16). Based on the proposition that a shared cultural, ethical, and moral space is required for a functioning community between two or more individuals (ibid.), scientific knowledge seeking in this quadrant asks how to shape and influence a coexistence that is conducive to growth for all individuals. "This intersubjective space (our commonly shared background contexts and worldviews) is a crucial component of the human being, without which our individual subjective identities could not even exist, and without which objective realities could not even be perceived." (Wilber, 1997, 17).
The methodologies of the external-collective quadrant are again empiricist and positivist; many fields of sociology, economics, and especially systems theory are typical scientific traditions in this quadrant. In keeping with the empirical methodology, the validity claim of this quadrant is the functional fit. "And it is the objective behavior of the overall social action system, considered from an empirical stance, that forms the yardstick by which truths in this domain are judged." (Wilber, 1997, 16).
Based on the validity claims, the following section describes the quadrants with the zones as expressions of inside and outside views of the respective object.
3.2.2 Methodological pluralism: quadrants and zones
In his most recent work, Wilber (2006a) additionally differentiates the quadrants, especially with regard to scientific ways of knowing, into an inside view and an outside view from which the phenomena of the respective quadrant are perceived (for details cf. Wittrock, 2008) and names these eight emerging perspectives as zones (Wilber, 2006a), to which he vicariously assigns certain methodologies, as exemplified in Figure 9.
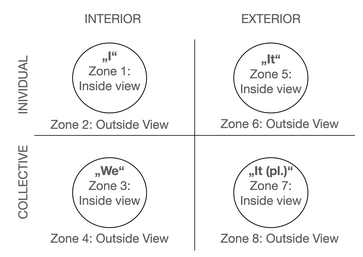
It should be noted in the illustration in Figure 9 that the numbering of the zones (following Wilber, 2006a) follows first the two left-sided, i.e., inner quadrants, then the two right-sided, outer quadrants, whereas in all other contexts of the quadrant model in Integral Theory, also in many of Wilber's publications (2001, 2006a), the upper, individual quadrants are addressed first, then the lower, collective quadrants. In short: In the case of the zones, the numbering runs first to the left, then to the right; in all other contexts, the consideration usually follows the order first above, then below. With the exception of this chapter, this thesis also follows the latter order.
3.2.2.1 Methodologies of the inner-individual dimension
Research in the upper left quadrant deals with the inner experience of individuals and thus faces the challenge that the structures to be researched are nowhere visible in the external world (Wilber, 2006a). This challenge is particularly evident in the first zone, because in zone 1 research is concerned with the inside view of the internal phenomena of an individual holon. The exemplary methodology of this zone is phenomenology, but introspection, meditation, or contemplation are also considered methodologies of this zone (Wilber, 2006a). Zone 1 insights are often gained from the exploration of states of consciousness. "All of these methodologies consider objects in the stream of consciousness as they show themselves." (Wittrock, 2008, 49, emphasis in original). From the point of view of representatives of right-sided, empirical research, this area diminishes the scientific claim of Integral Theory, since here (scientific) knowledge resides in the subject itself, and comes about neither through objectifiable criteria nor through the evaluation of the researcher himself. Instead, the researcher or investigator here is the individual himself or herself, looking at him or herself.
The larger area of scientific research in the inner, individual realm wants to make the non-visible visible, graspable for research in some form, and thus mostly makes use of an external perspective on the inner experience of the individual holon. This area of research Wilber calls Zone 2 and assigns structuralism to it as a proxy methodology. "When you research them [these realities], you are looking at them “from without,” you are not necessarily experiencing them from within." (Wilber 2006a, 54). Internal processes and operations of the individual, such as value orientation, religious orientation, emotional development, etc., are thereby assigned by the researcher (or the subject observing him/herself from the outside) to certain structures that contain different levels of manifestations of the respective process. Typical structuralist approaches exploring this quadrant include Kegan's work on consciousness development (Wilber, 2006a), Gilligan's approach to female morality (Wilber, 2000), and Graves' Spiral Dynamics model of individuals' value development (Beck & Cowan, 2008, cf. Section 3.1.3). It is also the zone that is invoked as an example of developmental lines in many of Wilber's works (2000, 2006a, 2009). Explored are the structures that individuals follow in certain internal phenomena, "one describes what invisible rules are obeyed by the phenomena that show themselves as phenomena to consciousness as 'immediately given'" (Wittrock, 2008, 51). In Zone 2, simply put, researchers assign an individual's inner experiences to particular levels of a structural model.
3.2.2.2 Methodologies of the inner-collective dimension.
From the inner-individual aspects, the model turns to the inner-collective aspects of a holon with zone 3, which is about the scientific consideration of the inner perspective of the inner experience of a collective holon. Hermeneutics is named as the guiding methodology of this zone, which is concerned with describing the 'felt we', the space of intersubjectivity. "But the subject matter is this actual we of understanding." (Wilber, 2006a, 157). Intersubjectivity, that is the emotions, thoughts, insights, and values shared by a group, or at least the vast majority of its members, where a single individual could never feel this 'we', could not have these experiences, without the fellow members of his group. As a researcher one takes part in the inner experiences of the group and has to understand the experiences in a hermeneutic circle, because only from the inside the 'we' can be grasped.
But from the inside, that we is a felt meaning, a conglomerate of signifieds, not a syntax but a semantics, not a structure but a yearning, not a grammar but a space of shared feelings and visions and desires and conflicts, a vortex of love and disappointment, obligations and broken promises, mutual understanding and devastating betrayals, the ups and downs of almost everything you call “important” in life, these webs of felt relationships (Wilber, 2006a, 156)
The external view of the internal experiences of a collective holon is the subject of Zone 4, for which Wilber cites ethnomethodology as an exemplary methodology. "Ethnomethodological research provides precise descriptions of the methods used by members of a society, group, or community to do whatever it is they do." (de:Wikipedia, Ethnomethodology). Wilber (2006a) further cites archaeology, genealogy, cultural anthropology, post-structuralism, and semiotics as examples. All fields and methodologies aim to capture and systematize the 'felt we' in namable categories and structures (grammar, syntax, etc.).
A more obvious and mundane example is ethnomethodology, which deals with the underlying codes, conventions, and rules of social interactions, and which is listed [...] as represantive of zone
#4, as long as it is understood that all sentient beings, not just humans, have an ethnos or ocial grouping. (Wilber, 2006a, 155)
To the 'we' from an external perspective, Wilber ascribes the status of something difficult to see, something that is mostly grasped only in terms and categories of a 'they', that is, from an external collective perspective, but which ignores the internal components, the 'felt we'.
The inside of a we can be felt, but the outside of a we has to be seen from a distance, and then over time, in order to grasp its full significance and structure. (Wilber, 2006a, 161f.)
Describing intersubjectivity from the outside requires the researcher to participate in the group itself, to experience the inside perspective of the we, in order to then describe the patterns of interaction in terms of categories and structures from the outside.
3.2.2.3 Methodologies of the external-individual dimension
The interest of the sciences assigned to the right-hand side in the quadrant model lies in observable processes and objective data, whose fascination, in Wilbers opinion, is particularly due to the simplicity of the assumptions associated with them.
I see sensorimotor objects out there; those objects (and probably those objects alone) are real; therefore true knowing consists of following the behavior of those objects as carefully as I can: that is, true knowing consists of making an accurate map of a pregiven nature. (Wilber, 2006c)
In the upper right quadrant, zone 5 describes the external phenomena of an individual holon from the internal view. As a representative methodology, Wilber mostly mentions autopoiesis according to Maturana and Varela (1987), which attempts to describe from an organism's inside how it develops or generates itself. This form of scientific knowledge is clearly different from the prevailing empirical methodology of Zone 6, which describes from the outside, and forces the researcher to adopt a quasi 'organic-empathic' attitude without having a dialogical access to the object of research.
This is the fundamental difference between classical behaviorism and autopoietic behaviorism. The former looks at the objective organism from without (zone #6), the latter, from within (zone #5). (Wilber, 2006a, 170)
The world of the holon under investigation is no longer described from the conceptualisations of the surrounding system (which is represented by the scientist), but an attempt is made to reconstruct the holon's world view from the organic circumstances (many olfactory cells in an animal species indicate an olfactory world enactment, i.e., a reconstruction of a world that consists more of olfactory signal stimuli than of visual signal stimuli).
Note that here, too, it is assumed that the biological organism 'stages' its world as an autopoietic system, i.e., it does not simply take in 'the world' via the senses, but co-creates the experience of its specific surrounding world. (Wittrock 2008, 57)
Other methodologies in this zone are, for example, sociobiology or neurophenomenology, in which the activity in certain brain areas is used to infer certain experiential contents without the subject himself being questioned.
In Zone 6, also located in the upper right quadrant, empiricism is the predominant methodology, which explores the external phenomena of an individual holon from an external perspective. This perspective dominates the current scientific landscape, which is critically noted by Wilber (2006a). This influential area of research is important according to integral understanding, but its importance is overestimated by the traditional science establishment, Wilber (1997, 21f) speaks of flatland reductionism, which reduces cognition to the perspective of the third person, the 'it' (or 'they') and ignores the perspective of the first person. In the field of consciousness research, scientific fields in this quadrant include neuroscience, which uses magnetic resonance imaging and positron emission tomography to investigate the structure and states of the brain (Wilber, 2006a), but also physics, chemistry and biology.
3.2.2.4 Methodologies of the exterior-collective dimension
The area of exterior-collective phenomena, bottom right, is devoted to patterns between objects (Wittrock, 2008) in contrast to the patterns between subjects observed in the lower left quadrant (zones 3 and 4). The lower right quadrant is first represented by zone 7, which reflects the interior perspective on the external processes of a collective holon. Wilber cites Luhmann's social autopoiesis, "the view from within" the social system (Wilber 2006a, 174), as the central methodology, whereby primarily the interactions between the individual holons of a social holon are considered in their development from within themselves. "The transfer of the concept of autopoiesis [by Maturana and Varela, 1987, cf. ch. 3.2.2.3, B.W.] to the phenomenal field of the social has the consequence that social entities are described as closed operating units that generate and maintain themselves by means of the recursive production of their elements." (Kneer & Nassehi, 1993, 65). According to Luhmann's understanding (Kneer & Nassehi, 1993), possibilities of intervention on the system from the outside are thus extremely limited. Science in this understanding does not so much look for ways of influencing the system, but rather gives a description of the mechanisms of self-preservation even under environmental influences, also with the background of showing risks and dangers of (self-referential) development.
Zone 8, the external view of the exterior phenomena of a collective or social holon, is finally the research sector of classical systems theory. Here, the structures and manifestations of the interactions of individuals are described from the outside, from an objectifiable point of view, in terms of their relevance to the system. "A social (LR) holon is composed of its members plus their exchanged artifacts." (Wilber, 2006a, 174). The focus of scientific interest is on processes, control loops (cybernetics), functions and structures that are necessary for system maintenance or system change (Miller, 1999). The individual is only relevant in its functionality and fit into the system. Integral Theory, for example, names chaos theory as a representative of this zone (Wilber, 2006a), which can be supplemented by the various systems theory approaches in economics and the social sciences.
3.2.3 The three strands of knowledge
The so-called three strands of knowledge are the steps of injunction, apprehension and confirmation familiar to all established sciences (Wilber, 2001a, 90), which are valid for science in all four quadrants. The scientific process of knowledge always begins with an instruction, a prescription, the injunction, as to how the data collection is to proceed. Types and forms of experimentation diverge: For the comparison of meditation experiences, there must be agreement on the procedure regarding meditation practice, framework conditions and others. For testing the effectiveness of medicines or other substances, standardised test series must be carried out. For the observation of culturally specific behaviours of people with dementia, field research must be conducted according to defined procedures. And for the comparison of health care systems, certain data must be collected in defined contexts after prior planning. Each zone has its own methodological specifications that determine the type and implementation of injunction, data processing and verification.
Perception takes place through data collection in the experiment, which can also consist of self-observation in the upper left quadrant in accordance with the injunction. These data can be of different natures according to the overarching methodology (zone). "All good science - narrow or broad - is to some extent anchored in data or experienced evidence." (Wilber, 2001a, 90). The rules of the epistemological path, whose injunction is determinative of the data, also apply to the processing of the data obtained (Wilber, 2001a).
The final step is verification, which involves refutation or confirmation of the initial thesis. Through the injunction, the basic procedure of gaining knowledge is repeatable and verifiable for all to a certain extent.
A community of peers—or those who have adequately completed the first two strands (injunction and data)—is perhaps the best check possible, and all good science tends to turn to a community of the adequate for confirmation or rejection. (Wilber, 2001a, 75)
If this is transferred to practical research areas, deviations are to be expected here: While a simple memory test with prepared test material is relatively easy for most users to perform, meaning that the injunction can be followed by as large a group as possible, this is more difficult in studies on meditation practice, which is based on highly individual mechanisms that can hardly be influenced from the outside. However, since there are also different validity claims for all four areas of effect, it ultimately makes no difference whether data are obtained from a memory test or a meditation experience, as long as they do justice to the validity claim of the respective quadrant.
Thus, the three strands of knowledge apply to science in all quadrants with their corresponding validity claims. Strictly speaking, the three strands must also take into account the different levels of development, for example of the researchers involved, the surrounding system or similar. The application of the injunction by a meditation novice will yield different results than that of a Zen master (levels of development), people with a highly developed cognitive and moral development lineage may evaluate interviews on moral judgements differently than cognitively less developed persons (lines), men and women may have different perceptions when applying an experiment and come to different results due to different contexts of experience (types) and finally the states must also be taken into account in an integral path of cognition: In which state did the observance of the injunction occur? In meditative contemplation, in a dream or in a waking state?
To be considered in the three-step approach of integral research are the three principles of Integral Methodological Pluralism (Wilber, 2006b). Non-exclusion means the fundamental willingness to recognise in every contribution a relevance to the issue being researched, even if it may be very small ("no human mind can produce 100 % error", Wilber, 2006b, 22). Unfolding is understood as taking into account the holarchical principle of inclusion and transcendence also in the generation of new knowledge, which also means questioning old paradigms and allowing for new ones (Wittrock, 2008). Finally, integral research requires attention to precise staging, i.e. attention to injunctions, to the specifications of the respective methodology, so that within its validity claim the corresponding data can be reproduced (Wilber, 2006b).
3.3 Summary: Integral research
To summarize, Integral Theory requires an integral research process to include as many structural elements as possible in the scientific knowledge process.
The injunction of Integral Methodological Pluralism requires the orientation of the object of knowledge towards the structures of the quadrants (ch. 3.2.3) or dimensions, taking into account
different validity claims. Injunction also requires the object of knowledge to be differentiated according to the various lines (ch. 3.1.2) in which development takes place across different
levels. The characteristics of development at the various levels (ch. 3.1.3) of the respective lines must also be described. Finally, the integral approach, which distinguishes between different
typical (ch. 3.1.4) and temporary states (ch. 3.1.5) and influenced by temporary conditions.
Linking all of these aspects together and showing cross-connections as transparently as possible is what constitutes scientific work with the integral approach. The principle that no findings
should be excluded (non-exclusion, cf. ch. 3.2.3) applies here; furthermore, the willingness to question traditional methods and paradigms in order to generate new knowledge (unfolding, cf. ch.
3.2.3) is a prerequisite for integral research. The ways in which data is collected using various methods (perception, cf. ch. 3.2.3) must be designed in such a way that a review is possible as
the final step of the research process.
Based on this theoretical approach, the following chapter discusses basic concepts and assumptions that are relevant for the application of Integral Theory on dementia.
4 Key assumptions for an integral dementia concept
In the previous chapters it became obvious that there is a lack of comprehensive dementia concepts (cf. ch. 2.2), combined with a dominance of the dementia discussion by the medical-behavioral sciences (cf. ch. 2.1). This dominance is increasingly criticized by different groups, by experts (Whitehouse & George, 2009; Wissmann & Gronemeyer, 2008), but also by some persons affected by dementia (Taylor, 2008).
There is a multiplicity of diagnoses, criteria, forms of therapy, approaches to care, and opinions, with no validated evidence to date on the causes of dementia (Wissmann & Gronemeyer, 2008). A significant use of cross-connections and synergies of different findings seems to be tedious up to almost impossible. This confusion of data resulted in the basic assumption that led to the topic of this thesis: So far, there are few dementia concepts whose framework is broad enough to link as many different findings on dementia as possible in a meaningful way and to clarify their interrelationships in a structured way. There is a lack of an overview, a metatheory in the sense of an overarching theory that brings together the existing findings.
Furthermore, it was shown above that the integral theory offers a framework to describe an issue comprehensively from a scientific point of view, taking into account previously conflicting viewpoints (cf. ch. 3).
The essential hypothesis of this thesis is that the Integral Theory is suitable to develop an integral dementia concept based on its structural elements and specifications of the Integral Methodological Pluralism, which is so comprehensive that a large number of findings on the entity dementia can be linked and integrated within the conceptual framework. Therefore, the aim is to create a draft for an integral dementia concept that provides a basic framework for a description of dementia according to integral criteria.
Viewing dementia from an integral point of view follows the claim of what Integral Theory wants to be: a 'theory of everything' (Theory of Everything, Wilber, 2001a). If one takes this claim seriously, it is consistent to confront the Integral Theory with the challenge of not only being able to describe a forward-upward development of consciousness, but also the phenomenon of an apparently regressing consciousness on the basis of its structural elements. This will also be the special challenge of this thesis: To transfer a phenomenon of consciousness, which has or seems to have the regression of (cognitive) consciousness as a special feature, into an approach, which so far has mostly been characterized by working on the development of higher levels of consciousness (Wilber, 2006a).
However, before an integral dementia concept can be outlined on the basis of insights from the theory and practice of dementia care and dementia research, it is first necessary to draw the necessary consequences from integral claims and to examine which basic requirements an integral dementia concept must meet.
4.1 Holon dementia
Before applying the integral model to dementia, it must be clarified whether dementia is at all suited for an integral consideration, as one of its basic assumptions is that evolution always contains an increasing complexity of the entities concerned (cf. chapter 3.1). At first the concepts of dementia and evolution seem to exclude each other, since according to the predominant understanding of dementia there is always a regression in the context of this phenomenon: A regression of the cognitive abilities of people with dementia (Engel, Mück & Lang, 2009), increasingly also of their involvement and participation in society (Wißmann & Gronemeyer, 2008), and organically a regression of their neurons and brain (Holthoff, 2009). Even integral theorists assign people with dementia in the last stage to the lowest stage in their developmental model (Beck & Cowan, 2008; Wilber, 2001a). Simplification rather than increasing complexity seems to prevail here. How, then, can one describe a phenomenon seemingly contrary to the evolutionary principle with a theoretical approach that sees forward-upward evolution as the basic condition of its approach?
A first answer is given by a basic assumption of the integral approach, as formulated by Weinreich (2005) in his approach to an integral psychotherapy: "The integration of contradictory aspects of a level can only happen at any time from a higher level of development." (Weinreich, 2005, 28). Dementia is of a sort contradictory: regression (in the form of a neurodegenerative disease) happens in an environment characterized by development (in the form of increasing individual awareness as well as growing level of medical-neuroscientific research), without the causes of regression being really fathomed so far (Wißmann & Gronemeyer, 2008). Resolving this inconsistency of dementia will perhaps only be possible at a higher level of development that incorporates and transcends all current knowledge. Development toward greater complexity and depth, as is suggested by the integral approach, is therefore necessary in all areas to address the phenomenon of dementia.
Crucial for the relevance of dementia for an integral approach ultimately remains the fact that dementia is a process that also (but not only) takes place in a conscious, feeling person - in his body, in his consciousness, in his relationships and in his environment. The affected people remain people in the sense of independent persons until the end, even if there are ethically different limiting views about this (Wetzstein, 2005b). Thus, they are and remain holons, which are wholes and parts. Thus, dementia is a part of human evolution and human consciousness and can therefore be considered a holon.
However, dementia as a unique phenomenon can also be considered as a holon, if the focus is not on the 'disease' or dementia-related changes in an individual person, but on the phenomenon itself. Here, the focus is on dementia-related change, on what constitutes dementia and what is changed by dementia at each level (cf. Mahlberg & Gutzmann 2009a, among others, for the individual points):
- the single neuron that dies,
- which is part of a brain area whose functionality is increasingly limited and which eventually regresses,
- which is part of an individual that increasingly loses memory and much more due to these increasing changes,
- which in turn is part of a society that is constrained by that member's failure, social withdrawal, and need for care (where there is a shift here from the individual dimension to the collective dimension, which are "equivalent (but not identical) dimensions of each occasion." (Wilber, 2006a, 145)
4.2 Focus of this thesis
So, what is the holon to be considered? This is where the first challenge of the integral model becomes apparent, to provide a sufficiently deep framework for the complexity of a (supposed) disease such as dementia that can encompass all facets equally. If one sticks to the medical definition of the term, it is possible to focus on a single form of dementia, which, as shown in Figure 10, would be represented in the quadrants as follows:
![Fig. 10: Aspects of the exterior-individual quadrant as an independent holon [1]](https://image.jimcdn.com/app/cms/image/transf/dimension=545x10000:format=png/path/sc9048d7fd3b8bac7/image/i0c2eafd054ebd957/version/1710962752/image.png)
If, on the other hand, the focus is placed on the individual person with dementia as a holon, the relevant aspects in the quadrants shown in Figure 11 arise:
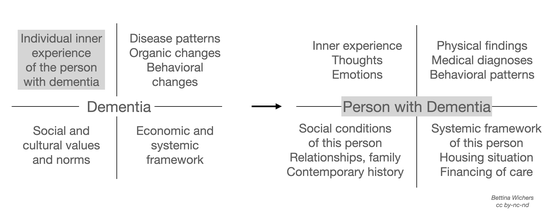
However, with the approaches shown in Figures 10 and 11, one remains caught up in individual aspects of the phenomenon of dementia, in the first case placing a medical diagnosis of the upper right quadrant, and in the second case focusing on the patient in his or her individual as well as social relations. A further focus would be the consideration of dementia in a religious community (as an aspect of the interior-collective quadrant, cf. Fig. 12) or in the system of old people's homes (as an aspect of the exterior-collective quadrant, cf. Fig. 13).
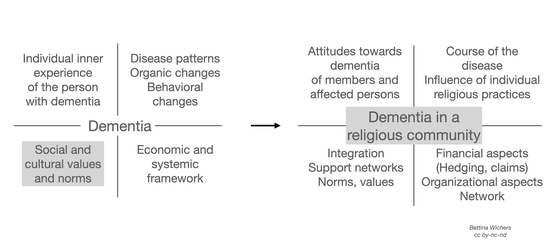

However, the aim of this thesis is a dementia concept that is more far-reaching and offers space for many other aspects of dementia: semantic meaning, cultural reception, personal experience of people with dementia, subjective external perception of relatives, organic development and medical diagnoses, insurance law and financial significance, ethical relevance and political positions, pharmacological therapies or nursing care concepts. Therefore, a comprehensive and at the same time delimited term of dementia must be defined as the basis of this concept.
[1] This and all following figures in this paper are the author's own illustrations.
4.3 Terminology
Dementia is seen in this work as a phenomenon around the clinical pictures of dementia as defined by the ICD-10 of the WHO (DIMDI, 2010) in all its cultural, systemic-organisational, individual and organic references. For this thesis, dementia is explicitly not defined as a disease, but as a term currently attributed to certain organic changes and behaviours of affected people associated with the ICD-10 criteria.
The definition of dementia in the ICD-10 is the basis of many standard works on dementia (Förstl, 2009a; Mahlberg & Gutzmann, 2009b), research projects and publications. It can currently be regarded as the only globally valid definition of the entity dementia, whose criteria, however, no longer correspond to the latest state of research (for discussion, see WHO, 2007). However, since the new edition as ICD-11, which is in preparation, is not yet known, this version will be the definitional basis of this work.
Dementia (F00-F03) is a syndrome resulting from a mostly chronic or progressive disease of the brain with disturbance of many higher cortical functions, including memory, thinking, orientation, comprehension, calculation, learning ability, language and judgement. Consciousness is not impaired. The cognitive impairments are usually accompanied by changes in emotional control, social behaviour or motivation, occasionally these also tend to occur. [...] (DIMDI, 2010)
From an integral perspective, it must be taken into account that in this case individual interior as well as exterior processes are defined by an institution with worldwide influence, so the consideration must take into account the exterior-collective influence. Dementia is defined by a system that is based on knowledge from experts representing perspectives from all quadrants but is nevertheless always also subject to institutional constraints. In the case of WHO as a 'defining power', it should also be kept in mind that the institution is obliged to represent the interests and concerns of all people involved (Wetzstein, 2005a), and therefore, for reasons of validity of the definition for as many nations involved as possible, will always remain somewhat more general in its definition than a nationally oriented and more research-focused association (Wetzstein, 2005a) such as the American Psychiatric Association (APA).
Here the validity claim of the exterior-collective quadrant, the functional fit, becomes clear: a globally valid dementia definition must be sufficiently open that it is functional for all health systems involved. The dementia criteria of the APA's DSM-IV are more nuanced in this respect, since, as a primarily nationally oriented organisation, they can refer to a more restricted (though still culturally broad) group of people. Especially because of the worldwide validity of the ICD-10 criteria, these will be the basis of the work here.
A further literal definition of the term dementia will be omitted here, since any definitional approach already implies a determination of the focus of a certain path of knowledge. Through the ICD-10 definition, a pre-determination of a medical definition is already made; however, this contradiction cannot be resolved for the time being and thus the demand on the research process arises to consider this fact sensitively.
So far in this work, the term phenomenon has mostly been used as a description for dementia, but this also needs to be concretised in the sense of a precise meaning of the word: In this work, dementia is considered both in its appearance as a phenomenon and as a noumenon, i.e. both as the event accessible to sensory perception (de:Wikipedia, Phenomenon) and as the thought itself, the "to be known with the mind" (de:Wikipedia, Noumenon) in Plato's sense. In this way, both the right-sided (phenomenon) and the left-sided (noumenon) ways of cognition are taken into account in relation to the quadrant model. The entity in the philosophical understanding of the term, which is defined as "unspecified existence of something" (de:Wikipedia, Entität), is chosen here as the overarching concept. Understanding dementia as an entity therefore means recognising it as 'something that exists' without being able to determine its nature. Such an open definition makes it possible to break away from previous definitions and to really openly include all aspects, the measurable as well as the conceivable.
The term quadrant or dimension, which Wilber usually uses synonymously (cf. ch. 3.1.1), also needs to be clarified. In connection with the entity of dementia, the dimensions of dementia appear to be the linguistically more intuitive terminology than the quadrants of dementia. Therefore, in the further course of this work, the term dimension is usually preferred to the term quadrant.
Finally, a closer look at the term concept is still pending, which should characterise the content and outcome of this work. The term dementia concept is chosen with reference to Wetzstein (2005a), in whose study the term was (re)introduced into the dementia discussion. In her study, she gives an overview of the substantive precursors of the dementia concept (Wetzstein, 2005a), but does not define the character and extent of a concept. There are also hardly any in-depth definitions to be found in the encyclopaedic literature. Meyer's Großes Taschenlexikon (1992) defines it as a "[keyword-like] draft, first version of a speech or writing, plan"; in Wikipedia, concept is described, among other things, as a 'first draft or as a preliminary stage of a theory' (de:Wikipedia, Konzept). Finally, the Deutsche Wortschatz [German Vocabulary] of the University of Leipzig (Deutscher Wortschatz, 2011) offers as a synonym, among others, model of thought.
If one summarises these definitions and synonyms and transfers them to the framework at hand here, a dementia concept can be defined as a thought model as a preliminary stage of a theory. An integral dementia concept is therefore understood in this work as a model of thinking about the entity of dementia based on Integral Theory.
Based on the explanations of the terms, the following section now presents the epistemological research framework of this thesis.
4.4 Epistemological research framework
According to an integral understanding (cf. ch. 3), all ways of knowledge that can be assigned to one of the four quadrants and that have a stake in the description and research of the entity of dementia are admitted in this work. The aim of an integral dementia concept is also the integration of different areas of knowledge, so that not only scientific research results, but also the knowledge of non-scientific professions, representatives of relatives and above all the people with dementia themselves, furthermore, for example, media contributions of different kinds (literature, films, websites) and experiences of different groups of people with dementia are to be included. Relevant for the inclusion of the findings and results of a person, group or institution involved is first of all not the scientific quality, but the question of whether the findings meet the validity claim (ch. 3.2.1) of the respective quadrant. The ideal of an integral dementia concept would thus be an overall picture of the entity of dementia that includes all currents and appreciates the shares of each contribution.
In order to test the thesis of the suitability of Integral Theory as a model for an integral dementia concept stated at the beginning of the chapter, two steps are taken. In a first step, an integral dementia concept is to be developed in its basic features, which is then to be tested in a second step for its scope in the sense of openness to as many insights into dementia as possible. The methodological details of both steps will be explained in more detail below.
4.4.1 Procedure for the development of an integral dementia concept
In the first step of the theoretical development and review of an integral dementia concept, a blueprint for an integral
dementia concept will be developed in chapter 5 from the basic principles presented in the preceding chapters. For the first section of the methodology, criteria for a dementia concept based on
the integral approach are formulated below, considering the implications of an integral methodological pluralism (ch. 3.2).
- An integral dementia concept should bring together findings on the entity of dementia from the relevant methodologies/zones from all quadrants of the Integral Theory (cf. ch. 3). Where possible, the interconnectedness of these four perspectives should be shown.
- An integral dementia concept should include relevant lines, levels, types and states of dementia in all quadrants as comprehensively as possible.
- An integral dementia concept should also include not only the entity of dementia itself, but also the perspective of as many stakeholders as possible (people with dementia, relatives, caregivers, researchers).
For the development of an integral model of thought or an integral concept, the following questions, which arise from the implications of the structural elements and the Integral Methodological Pluralism, offer clues for the scientific approach:
- What are the subject areas in this quadrant?
- Which scientific fields, disciplines, professions and institutions have their focus in the epistemological pathways of this quadrant?
- Which lines are differentiated in this dimension? How is this done?
- What other lines are thinkable in this quadrant?
- Which levels show up in this quadrants?
- Which levels can be relevant beyond this? What connections can be possible to other lines and levels?
- Which typologies can be found in this areaa?
- Which typologies are further conceivable in this area?
- Which states are considered by the respective methodologies?
- Which states are still possible in this quadrant and have not yet been considered?
- What correlations with other areas are evident in the respective quadrant?
For the design of an integral dementia concept, the questions regarding the quadrants and lines in particular provide the orienting framework. The spectrum of an integral view of dementia will be shown exemplarily on some lines of each quadrant and substantiated by data material from dementia research. For this purpose, online accessible sources from the databases GeroLit and Medline, some basic works of the current dementia literature (e.g. Förstl, 2009; Mahlberg & Gutzmann, 2009) and sources from the publications of the Kuratorium Deutsche Altenhilfe and the Demenz Support Stuttgart will be used to a large extent.
The integral approach with its multi-layered structural elements bears the danger of losing the common thread in the diversity of perspectives, lines and levels. Therefore, this work will be guided by the following ranking of structural elements:
- Quadrants as the top structural element,
- A number of exemplary lines as areas of development within the quadrants,
- Overview of some levels, states and typologies,
- Overview of zones as areas of different methodologies
The focus of this paper is thus within the quadrants on the exemplary presentation of some lines of development of the entity dementia. Individual examples of levels, typologies and states are added. The presentation of a possible relevance of the zones concentrates on an orienting overview.
Subsequently, dementia is largely considered in the cultural and systemic structures of the Federal Republic of Germany. A few examples from Scotland or the USA complement this, if there are no equivalent findings or structures in the German-speaking world or scientific field. Additional differentiation according to different cultural and systemic aspects (insofar as they transcend cultural diversity within Germany) is dispensed with here.
4.4.2 Procedure for reviewing an integral dementia concept
The thesis that an integral dementia concept provides the theoretical framework for incorporating a wide range of knowledge about dementia into its structure as comprehensively as possible will be examined in Chapter 6.
For this purpose, the data of a sample of publications on dementia from a scientific database will be categorised and evaluated with the help of a literature analysis. The categories will be formed using the structural model of the quadrants of Integral Theory, based on the insights gained in Chapter 5 about the basic structures of an integral dementia concept. The thesis linked to the main thesis of this thesis, that an integral dementia concept offers a range with which different insights into dementia can be included and linked as comprehensively as possible, is to be examined. Methodologically, this scope will be tested by examining in detail whether each publication of any sample of dementia literature can be assigned to at least one dimension of an integral dementia concept.
It will also be examined which relations become visible between the data obtained in the respective quadrants and whether the dominance of medicine over the dementia discussion discussed in chapter 2 and claimed by various authors (Wetzstein, 2005; Wißmann & Gronemeyer, 2008) can be represented with the help of the integral model.
The following chapter, however, is first dedicated to the development of an outline for an integral dementia concept.