
A Draft for an Integral Concept of Dementia
Translation of my Masterthesis in Gerontology (M.Sc.) at the University of Erlangen, 2011
"Entwurf für ein integrales Demenz-Konzept"
Note: Most of the text was translated with Deepl Pro and proofread afterwards. I have read Wilber in German, I apologize for imprecise translations of certain
integral terms into English. All German citations are translated with deepl.com from the original if not mentioned otherwise. The English citations should now be all original. Please note also,
that this is a corected version of the master thesis in that sense, that I corrected or adjusted all quotations with errors, which I have to confess that I have found some in the original, when I
was looking up the original English citations.
Table of content
5 Draft for an integral dementia concept
5.1 Interior-individual dimension of dementia
5.1.1 Lines
5.1.2 Levels, states and typologies
5.1.3 Inner and outer view of dementia in the interior-individual dimension
5.2 Exterior-individual dimension of dementia
5.2.1 Lines
5.2.2 Levels, states and typologies
5.2.3 Inner and outer view of dementia in the exterior-individual dimension
5.3 Interior collective dimension of dementia
5.3.1 Lines
5.3.2 Levels, states and typologies
5.3.3 Inner and outer view of dementia in the interior-collective dimension
5.4 Exterior-collective dimension of dementia
5.4.1 Lines
5.4.2 Levels, states and typologies
5.4.3 Inner and outer view of dementia in the exterior-collective dimension
5.5 Summary: Core Structures of an Integral Dementia Concept
6 Empirical evaluation of the integral dementia concept
6.1. Results of the literature analysis
6.2 Summary of the findings
6.3 Evaluation
7 Integral Theory as the Basis for an Integral Dementia Concept. Concluding Discussion
Bibliography
5 Draft for an Integral Dementia Concept
In this chapter, a draft for an integral dementia concept will be sketched on the basis of the Integral Theory presented in chapter 3 and on the basis of the essential assumptions and methodological procedures described in chapter 4.
If all fields of science have their equal share in explaining reality (cf. ch. 3.2), then an integral dementia concept must offer the theoretical space to integrate all the sciences and approaches involved and to place them on an equal footing. If one wants to represent dementia in all dimensions and perspectives, it is necessary - as shown above - not to focus on individual aspects of dementia, but on the entity itself.
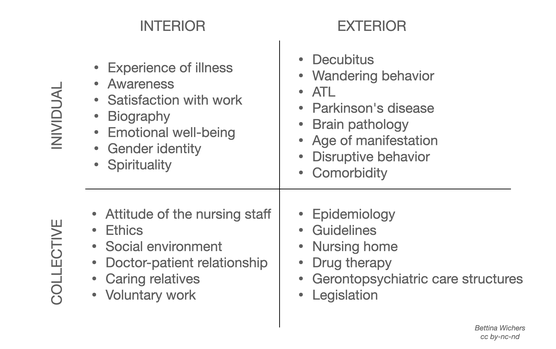
For the respective quadrants, the leading sciences listed in Figure 14 can be identified as an overview.
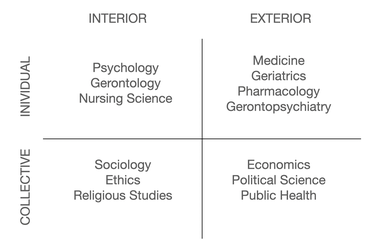
In the following, the consideration of the entity dementia runs along the sequence from the upper left to the upper right quadrant, then from the lower left to the lower right quadrant, i.e. from the individual to the collective aspects of dementia.
5.1 Interior-individual dimension of dementia
In the interior-individual quadrant, data is obtained from the inner experience of individuals, using multiple ways of knowing such as "meditation and contemplation, introspective psychology, psychoanalytic endeavours, shamanic journeys, the phenomenology of attention, dream analysis and bodywork" (Wilber, 2006c, 191). Knowledge about the interior-individual perspective of dementia is generated by psychology and gerontology, but also by geriatric care and caregivers themselves, increasingly supplemented by autobiographical accounts of people with dementia as well as relatives.
The interior-individual quadrant is about the experience of dementia from the inside with the validity claim of truthfulness (cf. ch. 3.2.3). Which feelings does a person with dementia have and how do these change in the course of the disease? What thoughts do people have about dementia? How do self-image and perception change in the course of dementia, of people directly affected, but also of accompanying relatives? What feelings do companions and other people involved, doctors, carers, neighbours, but also politicians who make health policy decisions, have about dementia? Dementia also 'exists' in them in the form of thoughts, fears, hopes and values. These perspectives of dementia are no less relevant, because they decisively shape the way dementia is dealt with and thus also the self-experience, thoughts and feelings of the people with dementia themselves (Kruse 2010).
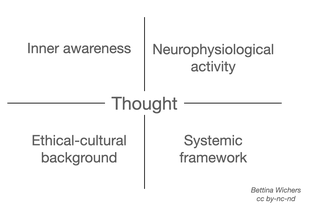
Excursus: Thought, considered integrally
According to Wilber (1997), thought itself is an inner process, a process of the mind or consciousness that is part of a person's inner awareness, but not an empirically observable process. What can be empirically recorded are the neurophysiological correlates, brain wave patterns, certain metabolic activities and behaviours, from changes in physiognomy to increases in blood pressure to concrete activities that can occur in conjunction with a thought.
We might eventually find that they are indeed two different aspects of the same thing, or that they are parallel, or dualist, or interactionist, or whatever, but the crucial point for now is that, in any case, neither can be reduced to other without remainder, because whatever else might be said, they each have a drastically different phenomenology. (Wilber, 1997, 10f.)
However, the collective quadrants are also involved in shaping the content of the individual thought, in that each thought of an individual is based on a horizon of experience that is shaped both by the surrounding society (inner-collective) and by the system (outer-collective) of which it is a part. An overview of the possible influences of each quadrant on the inner-individual process of thought is shown in Figure 15. The different perspectives are thus separate, but nevertheless interwoven: An inner-individual process must be seen and examined from its perspective (validity claim), but it is constantly subject to influences from the other quadrants and is thus ultimately a product of all quadrants (Wilber, 1997).
Now the point of this overall example is simply that my “single” thought, the original holon, is not really a single thought as such, but rather a holon with four inseparable aspects (intentional, behavioral, cultural, and social), each with its own validity claims (subjective truthfulness, objective truth, intersubjective justness, and interobjective functional fit). (Wilber, 2000, 145)
A differentiated consideration of thought as part of cognition in the context of the entity dementia is therefore advisable but can only be considered in a rudimentary way in this work. The assumption for this work is that the thought itself is an event in the inner-collective quadrant, which has correlates in all other quadrants (Wilber, 1997, 2006a).
The next section now provides an orientation on the dementia-relevant lines of the inner-individual quadrant.
5.1.1 Lines
This section describes the areas, the lines, where development takes place within the inner-individual dimension of dementia. Since the lines of this quadrant are theoretically well founded in Integral Theory (Wilber, 1997, 2000, 2006a), and since it is assumed that the areas of inner-individual consciousness do not differ fundamentally but only gradually under the influence of dementia changes, the guidelines of Integral Theory in this area can be used for an integral dementia concept.
Some lines of an interior-individual development, as outlined by Wilber in his various works (2001a, 2006a), are used as an orientation standard. Lines here symbolise the different areas of development of an individual in the inner realm (cf. ch. 3.1.2), which are deliberately not reduced to people with dementia, but also consider the perspectives of as many people involved as possible. Figure 16 shows examples of some lines of the Integral Theory that can also be relevant for the entity of dementia in the inner-individual realm.
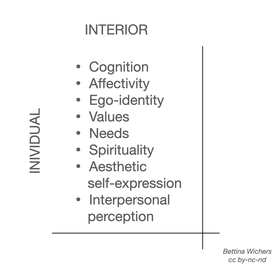
If the lines mentioned in figure 16 are applied to dementia, the following exemplary aspects of an integral dementia concept emerge:
The cognitive line asks how the respective person perceives what dementia is. What does the person perceive, what does he/she know about dementia, what are his/her thoughts about it? Findings on this line are available, among others, from research on the insight into illness of people with dementia (Engel, 2011), the insight and level of knowledge of spouses (Franke, 2005) or from research on "the phenomenon of 'professional resistance' to early diagnosis" (Pentzek, Fuchs & Abholz, 2005, 502) of GPs.
The affective line asks about the emotions regarding dementia. Among other things, autobiographical data from affected persons (Taylor, 2008; Zimmermann, 2009) and data from interview studies with affected persons (Engel, 2011) are available for this. For people in an advanced stage of dementia, the assessment instrument H.I.L.D.E. (Becker, Kruse, Schröder & Seidl, 2005) is a method for data collection. The emotional situation of relatives must also be taken into account (Engel, 2008).
For the line of ego identity with the question of understanding one's own self under the influence of dementia, insights arise from autobiographical testimonies (Taylor, 2008), but under certain circumstances also from the approaches of pre-therapy, whose aim is to enable severely dementia-modified people "to relate to themselves [...] again." (Pfeifer-Schaupp, 2009, 336).
For the line of value orientation, the Spiral Dynamics model is often used in Integral Theory (Wilber, 2001, 2006a). The relevance for dementia is shown in the exemplary naming of people with dementia for the lowest level of this developmental model (Beck & Cowan, 2008, Wilber, 2001a). However, the transfer of the orientation-providing value patterns of this model to people with dementia and other persons involved in dementia is still pending.
For the line of needs, Maslow's model of the pyramid of needs is mostly used (Wilber, 2006a). Data on the relevance of the levels of needs can be found in Höwler (2008) for relatives and companions of people with dementia. Kitwood's needs model (Kaufmann, 2010) is particularly suitable for assessing the needs of people with dementia.
The spiritual line asks about the spiritual needs of people with dementia (Müller-Hergl, 2007) or also of relatives (Radzey, 2007). The Spiral Dynamics model may also be relevant here, offering explanatory approaches to the spiritual needs of people with severe dementia (Küstenmacher, Haberer & Küstenmacher, 2011).
The line of aesthetic self-expression has to take into account, among other things, the aesthetic expressions of persons affected in their processing of dementia. Zimmermann (Quarks & Co, 2010), a person affected by dementia who discovered painting as a form of expression for himself, museum visits by people with dementia (Jonas, 2009) and the creative phases of well-known artists such as Willem de Kooning (Shenk, 2005), who also continued their artistic activity under the influence of a dementia-related change - these examples stand for aspects of an aesthetic dimension of dementia from within.
In the area of the interpersonal line of development, the focus is on one's own perception of interpersonal aspects under the influence of dementia. Sterin (2002) gives some indications of how dementia can express itself internally-individually on the interpersonal line for people with dementia. Kruse (2010) points out that a negatively or stressfully toned attitude of a person towards a 'dementia patient' can turn out to be a massive disturbance in communication, which the person with severe dementia also clearly feels.
5.1.2 Levels, states and typologies
For some of the lines mentioned above, levels can be identified that represent development over time in this area. Thus, for the lines of moral development according to Maslow (cf. Wilber, 2006a) and value orientation (Beck & Cowan, 2008), development over different levels is already implied. For the cognitive line, using the example of the insight into the disease [Krankheitseinsicht] of people with dementia, a development over time can be observed, which can extend from an awareness that something has changed, to an awareness that changes are 'not normal', to an awareness that the changes are a sign of dementia (Engel, 2011).
The severity of dementia according to ICD-10 (Förstl, 2009b), an objectively verifiable aspect of the external-individual dimension, can also be understood as a model of levels with an impact on the lines in the interior-individual dimension. A dementia process entails that, in contrast to the usual integral descriptions of developmental levels (Esbjörn-Hargens, 2009), no increasing levels of inner-individual depth or exterior-individual complexity are found here, but that with (objectively) increasing severity, a slowing down and deterioration of cognition are described on the basis of various cognitive abilities in the exterior-individual dimension (Förstl, 2009b; Engel, Mück & Lang, 2009). From the finding that "that consciousness develops in direct proportion to an organism's organizational complexity" (McIntosh, 2007, 174), the reverse conclusion can possibly be drawn that the decrease in the complexity of the organism represented by the objective degrees of severity could be associated with a decrease in the complexity of the inner-individual consciousness that can only be verified subjectively. However, no evidence can be presented for this thesis; it is presented here in the sense of a consideration of connections that have not yet been uncovered, as provided for in the methodology in chapter 4.2.
Exemplary for states in the internal-individual dimension is the state of orientation or disorientation with its four characteristics of time, place, situation and person (Engel, Mück & Lang, 2009), as well as the influence of neuroleptics (Wolter, 2009) and the time of day, e.g. in the sun-downing phenomenon (Mahlberg & Kunz, 2009), each of which can affect the various lines of this dimension, i.e. the various inner-individual abilities of people with dementia as well as other people, in typical ways that are not described in detail here.
In the typologies, the forms of dementia (Mahlberg & Gutzmann, 2009a), gender roles (for physicians cf. Groll, 2008; for carers cf. Neumann, 2009), but possibly also personality types can influence the expression of the respective line or ability.
5.1.3 Inner and outer view of dementia in the interior-individual dimension
Integral Theory distinguishes between two views of the object of investigation, for the interior-individual dimension phenomenology is usually named as the methodology of the inner perspective (Zone 1) and structuralism as the methodology of the exterior perspective (Zone 2) (cf. ch. 3.2.2.1). The methodologies mentioned in Integral Theory as generic terms for the zones (Wilber, 2006a) are followed in the awareness that these only refer generally to the principles of the respective zones (this also applies to the explanations of the zones in the other quadrants that follow later). However, they are considered sufficient for an overview of these zones.
Figure 17 gives an overview of both perspectives of the interior-individual quadrant and possible focal points of knowledge regarding the entity of dementia.
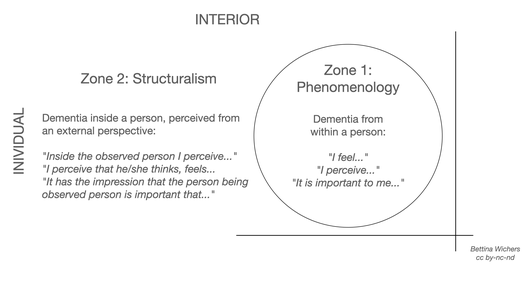
In the area of phenomenology (Zone 1), the aim is to capture the inner-individual being of dementia from the inner perspective of the individual (cf. ch. 3.2.2.1). Autobiographical accounts of people with dementia (Taylor, 2008), but also of other people from the context of dementia, can be regarded as data. Only a person affected by dementia (directly or indirectly) can give a true account from introspection of how dementia shows and feels from the inside. Phenomenological insight means that outside researchers or companions can hermeneutically interpret the reports of the person with dementia (who is the actual researcher in the integral sense, in that he produces the data material as a report from his inner experience) as individual testimony, but cannot measure and categorise it according to objective criteria.
The inner-individual dimension of dementia from the external perspective is collected using structuralist methods (Zone 2). The difference to the data of zone 1 is that the (qualitative) data of the subject, e.g. the person with dementia, about the inner experience, perception, moral judgement or aesthetic sensation of dementia are assessed and evaluated or interpreted by outsiders (carers, scientists) or by conscious self-observation on the basis of structures (e.g. categories, patterns, levels) (cf. ch. 3.2.1.2). Kitwood's needs model and its extension by Kaufmann (2010) are examples of structuralist methods in the context of dementia.
In summary, this brief overview of the two perspectives on the internal-individual dimension of dementia shows that the same set of facts (represented by the lines) can be viewed from different perspectives and that, from the point of view of Integral Theory, both perspectives must be given equal consideration, as they each have a part to play in establishing the truth.
5.2 Exterior-individual dimension of dementia
From the inner-individual experience of dementia, the interest now turns to the exterior-individual quadrant. The focus of (scientific) knowledge is dementia as it appears in the physical dimension of an individual: with the organic alterations as well as with the concretely observable behaviours. Most of the epistemological traditions of this quadrant are assigned to Wilber's zone 6, i.e. they look at the external-individual dimension of dementia from an external perspective and describe these processes in objective terms. In addition to medicine, the related neurosciences and the behavioristic psychology, the externally oriented aspects of the nursing sciences, pharmacy, and all related empirical sciences have their share in gaining knowledge for the external-individual domain, whose validity claim is truth (cf. ch. 3.2.1).
In dementia research, medicine is considered the leading science, and the research results from this sector have a high value in the scientific as well as practical consideration of dementia (cf. ch. 2). However, this high regard for the undeniably important medical findings often results in the phenomenon of quadrant absolutism (Wilber, 2007), i.e. the generalisation and overestimation of the data of one field and the associated marginalisation of findings from other epistemological traditions. Many researchers in this field see themselves in a battle against a "scourge of the 20th and 21st centuries" (Haass, 2006, 19), which can only be won through increased use of medical research. With the quadrant differentiation, Integral Theory gives medicine and its related sciences the space it can define, without this automatically resulting in a definitory influence on the areas of knowledge of the other quadrants.
Questions in this quadrant are: How does dementia manifest itself on an organic level? What processes, what changes can be observed? What kind of behaviours do people with dementia show? What is the specificity of dementia that can be objectively perceived and described? Dementia may also show itself as an entity in physical characteristics or behaviour of companions, relatives and other persons involved. For the description of the basic structures of an integral dementia concept, however, the elaboration will largely concentrate on the external-individual aspects of people directly affected by dementia.
5.2.1 Lines
Integral Theory names the following lines as examples for the external-individual quadrant: organic structures, neuronal systems, neurotransmitters, brainwave patterns, skeletal-muscular growth, nutritional intake and kinaesthetic capacity (Esbjörn-Hargens, 2009, 12). If one asks about the relevance of these lines for dementia, roughly three lines can be distinguished as shown in Figure 18, in which dementia shows up from the objectively perceptible dimension of an individual, here only referring to the objective factors of a person with dementia: In physical/organic characteristics, in abilities and in patterns of behaviour.
Deviating from the integral view of lines, three superordinate lines of dementia are seen in this quadrant, as shown in Figure 18, which can be differentiated into further areas. These are partly to be seen as partial aspects (i.e. 'lines of lines'), partly as level models. The question is whether the organism is to be understood as a level model (molecules - cell - organs - organism) of a single lineage, or as different lineages of bodily development extending over different levels (molecular processes developing at different tempos than cellular structures, which in turn are subject to different mechanisms than the development of different organs). It is answered here in favour of a model of several lines on which development is observed over several levels.

Numerous data are already available for the physical and organic line of dementia (Förstl, 2009a; Mahlberg & Gutzmann, 2009a). In the following, these are shown in a generalised manner for the entity of dementia, instead of being assigned to specific forms of dementia (Mahlberg & Gutzmann, 2009a) as is customary in medicine. According to integral understanding, the dementia forms are to be understood as types, not as lines of dementia, as will be explained further below. In empirical research, the following factors are found in the context of dementia in the external-individual quadrant (without claiming to be exhaustive):
- Molecular and cellular level: β-amyloid plaques, hyperphosphilated tau protein, Lewy bodies, prions
- Organic causes: Normal-pressure hydrocephalus, microangiopathies, tumours
- External factors: Alcohol abuse, poisoning, cranial injury, vitamin deficiency (Mahlberg & Gutzmann, 2009a)
These lines are influenced in their development by various conditions, such as drug therapies (Benkert, Hautzinger & Graf-Morgenstern, 2007) or time of day (e.g. sun-downing phenomenon, Mahlberg & Kunz, 2009). Furthermore, the expression of these factors depends on typologies such as sex types (Neumann, 2009), dementia forms (Mahlberg & Gutzmann, 2009a) or genetic dispositions (Jessen, 2009b). Some of these aspects will be discussed in more detail in chapter 5.2.2.
The line of behavioural patterns of dementia can be differentiated with regard to the empirical data situation in this area using, among other things, the nursing-scientific theory of activities of daily living (ADLs) by Juchli (Köther & Gnamm, 1995). As an example, some data in this area are shown below for the ADLs "resting and sleeping", "moving" and "communicating" (Köther & Gnamm, 1995).
The external-individual dimension of dementia becomes apparent in the area of resting and sleeping especially in the research around sleep disorders (Mahlberg, 2009) and circadian rhythm disorders of people with dementia (Mahlberg & Kunz, 2009).
The activity area of moving shows data from various sources, from cycling tours with dementia patients (Schabacher, 2011) to the scientifically evaluated combination of memory training and psychomotor training of the SimA programme (Oswald, 2004). In this topic, the cross-connection to another aspect of the external-individual dimension of dementia, which is not considered further here, is obvious: Movement is one of the factors that, according to numerous studies, has been shown to be a preventive factor for dementia (Müller, 2008).
The activity area of communicating here refers to the ability of people with dementia to communicate. Numerous studies are dedicated to the area of non-verbal communication of people with dementia (Sachweh, 2009), furthermore, dementia also manifests itself on the external-individual level in particular in speech disorders such as aphasia and apraxia [source]. Due to the conditional nature of communication in advanced stages of dementia, an integral dementia concept should also take into account the communicative behaviour of relatives (Engel, 2006) or carers or companions in general (Powell 2009).
The line of abilities includes not only the aspects of sensory abilities such as hearing impairments (Jonas, 2008), but also a positive concept of abilities, as is evident, for example, in the offer of dancing afternoons for people with dementia in a dance school (Arp, 2011).
The results of people affected by dementia in dementia screenings (e.g. Mini-Mental-Status-Examination, MMSE, Engel, Mück & Lang, 2009) can also be seen as an expression of the line of abilities according to integral understanding. The ability to draw a geometric figure (Engel, Mück & Lang, 2009) is, from a medical-psychological point of view, a statement about the expression of the 'disease' or the 'disorder' of dementia, but according to integral understanding it is 'only' the expression of a certain ability of an individual person. The interpretation as a dementia diagnosis only comes about through the evaluation criteria set by the developers of the respective screening; without the underlying catalogue of criteria (an influencing factor of the external-collective dimension of dementia), the ability cannot be interpreted as an expression of dementia, even from the perspective of empirical science.
5.2.2 Levels, states and types
The level model of the severity of dementia has already been described in its influence on the interior-individual factors of dementia (cf. ch. 5.1.2). In the exterior-individual quadrant, an increasing degree of severity in a person with dementia is shown, among other things, in objectively ascertainable changes in the activities of daily living (Förstl, 2009b).
The abilities of people with dementia in dementia screenings (cf. ch. 5.2.1) can also be interpreted as level models. Certain abilities that are tested in a screening (e.g. certain linguistic performances, cf. Engel, Mück & Lang, 2009) characterise the areas in the individual in which dementia-related development takes place. These are represented by the test results as levels, i.e. models of development over time. Here, the challenge indicated in Chapter 4 of representing downward regressive development with the structures of a model oriented towards forward upward development appears.
The medicinal-pharmacological therapeutic options can be seen as one aspect of the states of dementia in the external-individual realm. For medical science one of the focal points of research, medicinal therapeutics show themselves from an integral point of view as state areas in which the entity of dementia shows itself differently. Drugs are not a line of the exterior-individual quadrant (they are not part of the individual), nor are they levels of dementia in the exterior-individual domain, because they are not part of the development of dementia over time, but have an external effect on this development. In their influence on dementia, they are therefore to be understood as "temporary occurrences of aspects of reality" (Esbjörn-Hargens, 2009, 12, cf. ch. 3.1.5), because they change certain molecular or neuronal patterns of the organism, but do not become part of it (cf. also ch. 5.2.3.1). Thus, the drug therapy of dementia, which takes up a large part of the attention in science and research, becomes one factor among many others in the view of the external-individual quadrant of the Integral Theory. However, it is an artefact of (collective) medical-scientific dementia research, and therefore has its own status in the external-collective quadrant (cf. ch. 5.4.1).
The types of dementia are one of the basic typologies of the entity dementia in the exterior-individual domain. They are a scientifically recognised differentiation model (Mahlberg & Gutzmann, 2009a) of the characteristics of the behaviour and organic changes of a person affected by dementia. Following Habecker (2010), the dementia types are to be understood as an expression of the variance of dementia processes on a horizontal level, i.e. they describe the numerous typical developmental paths of a dementia process, which always proceeds similarly, but with typical variations with regard to the lines, levels and states of this area. Types in this area that may need to be considered separately are the reversible dementias (Schulz, 2009). Other relevant typologies for the external-individual dimension of dementia may be gender types (Schmidt, Assem-Hilger, Benke et al., 2008) or genetic dispositions (Jessen, 2009b).
5.2.3 Internal and external view of dementia in the exterior-individual dimension
Also for the zones of the external-individual quadrant, the mentioned methodologies or scientific areas are only to be understood as examples, following the Integral Theory (Wilber 2006a). Figure 19 below gives an overview of possible questions of the internal and external view of the external-individual dimension of dementia (cf. ch. 3.2.2.3).
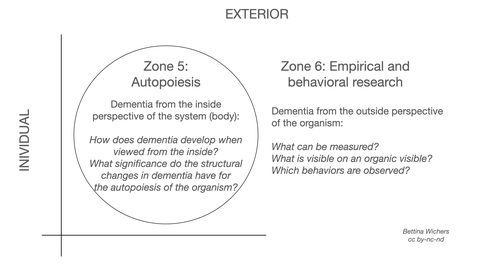
Since the theory of autopoiesis (zone 5) as a model for the internal view of the external changes of the individual (cf. ch. 3.2.2.3) has not yet been applied to dementia, only an orienting presentation of a possible relevance of this theory can be shown here without presenting the theory in detail. Maturana and Varela (1987) describe the nervous system as an operationally closed system that constantly 'produces' the world it perceives itself in such a way that it can only perceive those things for the perception of which it has also developed the structures. Changes in the environment of the human being (who, in contrast to the cell, is regarded as a so-called 'metacellular organism', Maturana & Varela, 1987) are regarded as perturbations (disturbances) that exist independently of the individual as part of the milieu in an operationally different system. Now, the living system (the individual) is not simply at the mercy of these factors, but determines whether and how it reacts to these perturbations, "it is rather the structure of the living being that determines what change occurs in it as a result of the perturbation." (Maturana & Varela, 1987, 106). The environment and the living being (as long as there are no destructive interactions) act as mutual sources of perturbation and trigger structural changes that serve the other system to maintain self-organisation, which is called structural coupling (Maturana & Varela, 1987).
A possible relevance of this theory for dementia arises from the following assumptions: Structural change of the whole organism occurs through the nervous system at the synaptic level (Maturana & Varela, 1987, 183), and these structural changes are fundamentally subject to the autopoiesis of the whole living being (ibid.). However, when the organism can no longer select the structural changes that enable it to continue to operate, it dissolves (Maturana & Varela, 1987, 187). Mechanisms such as apoptosis of nerve cells (Hessenauer, n.d.) can possibly be understood as mechanisms of dissolution within the framework of this theory, if the cell were no longer able to react to the perturbations of the environment with structural changes. The neuronal networks regressing through dissolution of individual cells would subsequently lead to a change in the experience of "the world out there", which in turn would affect the future perception of the world.
The empirical sciences (Zone 6), on the other hand, as representatives of the external view of the external-individual dimension of dementia (cf. ch. 3.2.2.3), observe and measure the objectively perceptible facts in the individual (in contrast, for example, to epidemiology, which looks at the manifestation of dementia in a population, which is an aspect of the external-collective dimension). What is considered as dementia is the result of observations of certain behaviour of a certain individual, some organic findings in combination with criteria defined by certain institutions (external-collective dimension). The empirical sciences, including medicine and behaviouristic psychology, focus on the objective measurement of these externally perceptible factors. All the data of the lines mentioned in section 5.2.1 originate from this field of knowledge, so that a further elaboration can be dispensed with at this point.
In summary, this quadrant shows the contrast between a so far unusual, partly unknown view of dementia in zone 5 and the known methods and data on dementia in zone 6, which are generally accepted in the scientific community.
5.3 Interior collective dimension of dementia
From the individual quadrants, the focus now turns to the collective aspects of dementia, the 'we' being at the centre here. The interest in knowledge is directed towards the inner processes of a collective, a community or society that is involved in dementia in some way. The data of this quadrant are obtained from the observation and interpretation of the norms, values, rules and intersubjective behaviour patterns of the respective community. The sciences involved are, in the broadest sense, cultural and social sciences (cf. ch. 5.3.3), which ask, for example, how dementia manifests itself on the interior-collective level, or which cultural forms of coping different societies develop. The perspective changes from an individually objective one in the exterior-individual quadrant to an intersubjective perspective of dementia, to an understanding description of the 'felt we' of dementia in zone 3 (ch. 5.3.3.1) or the systematisation, a description from the outside of precisely this felt 'we' in categories of the participating sciences in zone 4 (ch. 5.3.3.2). The validity claim of this quadrant is justice.
5.3.1 Lines
Relevant lines are also named for this area in Integral Theory: Worldviews, intersubjective dynamics, linguistic meaning, cultural values, background cultural contexts, philosophical positions and religious understandings (Esbjörn-Hargens, 2009, 12). Transferring these specifications to the entity of dementia, different lines can be identified as areas of the development of intersubjective dementia, as shown in Figure 20.
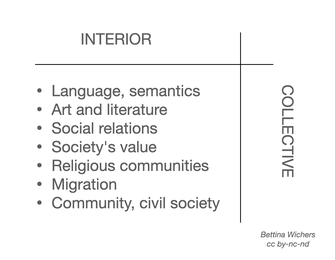
As examples, some areas will be outlined here on the basis of selected data, where the entity of dementia as a 'felt we' (cf. ch. 3.2.2.1) comes to light.
The line of language asks, among other things, about the semantic meaning of the term dementia. The emergence of dementia via the concept of senility and in conjunction with the concept of Alzheimer's disease is shown by Kreutzner (2008). Following a government initiative in Japan, a new formulation for dementia-related changes was found to replace the previous term with meanings of 'stupid' and 'mindless' with a term meaning "challenge to cognition" (Whitehouse & George, 2009, 65). Whitehouse & George's (2009) 'debunking' of the myth of Alzheimer's disease also falls within the linguistic lineage of the entity of dementia. The culturally defined terms for people who are 'afflicted' with dementia according to medical definitions are another expression of this lineage, as exemplified by the term "people with dementia" (Wißmann & Gronemeyer, 2008, 71).
Similarly, dementia is evident in the lineage of literature, where it is not the artifact of the printed work that is at issue (that would be an aspect of the external-collective quadrant), but rather the meaning content that the reader is able to access for him or herself, thus placing cognition in the realm of hermeneutic methodologies. A well-known example from the field of fiction is Suter's (1999) novel Small World; furthermore, two biographical publications by sons about their fathers affected by dementia (Geiger, 2011; Jens, 2009), among others, have recently attracted attention and increased public reception of dementia via literature. An overview of children's and young adult literature on dementia is provided by Jonas (2006). Also relevant in terms of conveying cultural meaning of dementia may be popular science publications on dementia, such as Jürgs' (2001) publication on Alzheimer's disease subtitled Spurensuche im Niemandsland [Searching for traces in no man's land], or Taylor's (2008) autobiographical exploration of dementia.
The lineage of social relations continues to provide numerous data on the 'felt we' of dementia. These can include, among others, the intersubjective aspects of care and support concepts that provide recommendations for shaping relationships with people with dementia (Engel, 2006; Feil, 1992; for other concepts, see Myllymäki-Neuhoff, 2009). Furthermore, data can be found on the intersubjective aspects of multiple relationships, such as relatives in general (Engel, 2007), spouses (Franke, 2005), or between grandchildren and their grandparents under the influence of dementia (Philipp-Metzen, 2008).
Another aspect that is still relatively unconsidered in research is the line of intersubjective relationships between people with dementia, where both situations of institutional living independent of care relationships would have to be taken into account, and also the relationships in self-help groups such as the Scottish Dementia Working Group (n.d.), whose organization is structured completely autonomously, i.e. without the influence of 'healthy' persons.
This list, as with the preceding dimensions of dementia, by no means reflects the state of knowledge from science, practice and civic engagement of dementia. It is therefore to be understood here only as exemplary for the range of representation of the entity dementia in the interior-collective quadrant.
5.3.2 Levels, states and types
By way of example, some of the lines of the previous section will be used to show how, from the point of view of an integral dementia concept, the findings in the various lines, i.e. areas of development of dementia, are also presented across various levels, i.e. stages of development. Likewise, some relevant states and types will be pointed out.
In the field of language, the use of the term "people with dementia" in the German literature (Wißmann & Gronemeyer, 2009), and in the English-language literature "people with dementia" (Ballenger, 2006), which increasingly replaces the use of terms such as "dementia patients" (Lind, 2000) or "demented" (Grond, 1997), can be understood as an expression of developmental levels. The meaning of the term further differentiates into different types of cultures and ethnic languages. Within these types, in turn, development takes place over time in the sense that the semantic meaning, the cultural interpretation of the "sign" of dementia has changed over time (cf. the situation in Japan; Whitehouse & George, 2009). Thus, we can speak of the individual languages as level models of dementia in the internal-collective quadrant, differentiated by type.
Some typologies of dementia have already become evident in the line of social relationships, for example, relationship dynamics differ, among other things, on the basis of relationship partners (types), for example, grandchildren or spouses as part of the relationship dyad (Franke, 2005; Philipp-Metzen, 2008). Possible states - a hypothesis to be tested for later research - could be, among others, wars or humanitarian disasters, which could potentially affect the integration of people with dementia in society.
5.3.3 Internal and external view of dementia in the internal-collective dimension
In the interior-collective dimension of dementia, too, a distinction is made between an interior and an exterior view of dementia (cf. ch. 3.2.2.1). Figure 21 gives an orienting overview of possible questions of the two zones with regard to a recording of the intersubjectivity of dementia.
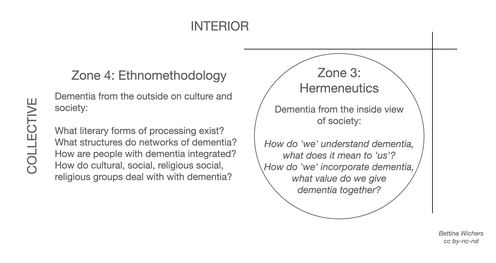
For a hermeneutics (zone 3) of the intersubjectivity of dementia it seems to be necessary to develop different constructs of hermeneutic understanding for the different 'cultures' of communities of dementia. If one follows Schnell's (2008) thoughts, dementia also needs to be considered as part of a distinct (dementia) society, since "dementia does not only mean deficiency, degradation, or loss of mind, it can also manifest itself in an otherness that extends to a different normality (Georges Cangilhem)." (Schnell, 2008, 80). Accordingly, a distinction must be made between, for example, intersubjectivity between persons not affected by dementia, in which dementia is a constituent or accompanying feature of the relationship, intersubjectivity between those affected and those not affected, as in everyday life in nursing homes, and intersubjectivity between those affected, taking into account both interactions between people with severe dementia in a nursing facility, but also interactions of people with dementia in a self-organized support group such as the Scottish Dementia Working Group (n.d.).
Ethnomethodology (Zone 4) is mentioned here as representative of the methodologies of an external view of the interior-collective dimension of dementia. Integral Theory gives few examples here that lend themselves to obvious application to dementia (Wilber, 2006a), ethnomethodology certainly offers starting points due to the relevance of the topic of dementia and migration. Orientation can further be found in Wilber's (2006a) characterization of ethnomethodology, which is "which deals wit the underlying codes, conventions, and rules of social interactions" (Wilber, 2006a, 154), which allows the cultural and social science data shown in Chapter 5.3.1 to be assigned to this zone.
In summary, these two zones reveal the patterns and relationships of respective social relations and meanings both from within the 'we', the 'felt we', and also from the external view of the 'we', the 'observed we'.
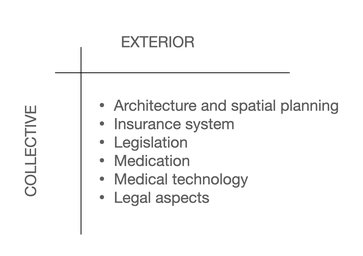
5.4 Exterior-collective dimension of dementia
For this final section of an integral dementia concept, the external-collective domain of dementia, objective, measurable data are collected on structures and artifacts of the system in which dementia is manifested. Participating scientific fields include economics, epidemiological health sciences, policy, and law. Also, findings from architecture or practice-based findings from interior design and garden design may be relevant to the representation of the entity of dementia in the external-collective quadrant. Further, this is the space of prevalence and incidence, of figures about the collective manifestation of dementia. The 'hardware' of medical-pharmacological sciences, which is developed for dementia diagnostics and therapy, further counts to this dimension.
An epistemic question in this field is how and where dementia is represented in the external-collective domain. According to the validity claim of this domain, the functional fit, it is asked where dementia has an impact and which structural adjustments are necessary to enable a dementia fit.
5.4.1. Lines
Also in this quadrant, dementia-related development takes place along many lines. For the exterior-collective domain, the integral literature points to geopolitical structures, eco systems, insurance systems, written legal codes, and architectural styles as characteristic lines of this dimension (Wilber 2001a, Esbjörn-Hargens 2009). From the scope of this quadrant, the functional fit, one can formulate as guiding questions: Where does dementia show up in systemic aspects? Where does dementia prove to be a functional, structural fit, where not? What is being done to achieve this fit?
The lines mentioned are also relevant in the field of dementia, but are to be further differentiated and supplemented, so that in this work the lines shown in Figure 22 are considered relevant for the external-collective dimension of an integral dementia concept.
The insurance system is a separate line of the system, in which dementia appears, as it has to develop necessary structures for a functional fit of all parts of the system (so also the people with dementia). In this context, dementia-relevant development is taking place in the areas of health insurance (SGB V, BMJ, 2011a) and long-term care insurance (SGB XI, BMJ, 2011b), among others. The different areas such as care benefits in kind (§ 36 SGB XI) and care allowance (§ 37 SGB XI) in home care for people with dementia are part of the system whose task is to provide structures to ensure dementia as a functional part of the system.
The line of legal aspects of dementia is dedicated, among other things, to the question of the general legal capacity of people with dementia (Schmoeckel, 2010) or the testamentary capacity of people with dementia in notarial matters (Lichtenwimmer, 2010). However, it must be noted that these are not 'capacities' in the sense of the upper right quadrant, but rather what is granted as capacities to people with dementia from a systemic perspective (lawyers being understood here as representatives of systemic structures).
Another line of the exterior-collective dimension of dementia is architecture, here related beyond the 'classical' retirement home to all (institutional) living concepts in which people with dementia are cared for. Approaches of architecture (Marquardt, 2006) and aspects of interior design such as the effect of lighting on people with dementia (Sust, 2009) are expressions of the system to 'fit' people with dementia into it. In the particular design of gardens (Rath, 2004) or in the simplest structural aspects such as the position of seating in recreation rooms of nursing homes (Strunk-Richter & Krämer, 2008), the influence of systemic structures on the entity of dementia becomes obvious in its interconnectedness with the other dimensions.
Finally, the structural data of dementia should be mentioned, as lines of epidemiological development (Ziegler & Doblhammer, 2009), in the field of cost development in the health care system (Kiencke, Rychlik, Grimm & Daniel, 2010) and the general socioeconomic relevance of dementia (Michel & Niemann, 2002). It is true for all factors that they represent areas of systemic development in whose structures dementia emerges. The area of medicinal therapeutics (Benkert, Hautzinger & Graf-Morgenstern, 2007) has already been discussed in the external-individual area in its influence as a temporary condition on the organism. This domain represents artifacts of the medical-technical system, as do the various imaging techniques (Holthoff, 2009); both aspects are independent developmental domains of the exterior-collective dimension of dementia.
Furthermore, guidelines (ICD-10, DIMDI, 2010; S3-Leitlinie Demenzen, DGPPN & DGN, 2009) and institutions (e.g., Demenz Support Stuttgart, 2010a.; Aktion Demenz, n.d. a) related to the entity dementia can be seen as expressing lines of dementia in the exterior-collective quadrant (as opposed to the meanings and value patterns they convey, which are line of the interior-collective quadrant).
5.4.2 Levels, states and types
As a level model of the exterior-collective quadrant, the development of the ICD criteria of the WHO can be considered. Comparing the development of the criteria over time, a change in the framework of the dementia entity can also be seen in these structures, including in discussions of the International Advisory Group on the ICD-11 catalog under preparation, which criticize the unsuitability of the mental illness criteria for nursing and health care (WHO, 2007, 3). The Advisory Group recommends a telescopic structure of the future criteria for nursing and health care as the lowest level, followed by further differentiated criteria for clinical use, on which further differentiated criteria for use in the research sector should be based (WHO, 2007). This would result in differentiated levels already in the definition of dementia, which could ensure improved applicability of the criteria in the respective sector.
Other level models can be found in the education and training sector of the nursing professions, recognizable among others by the "Levels of Knowledge and Skills" (Scottish Government, 2011), but also in the German training system for geriatric care with different qualification levels such as care assistants (GKV, 2008), certified geriatric care assistants (Land Hessen, 2007) and certified geriatric nurses (BMJ, 2009).
Nursing home architecture includes several areas where change can be understood as an expression of development over time, which could be based on changing requirements regarding a functional fit of aging and dementia in particular: In the area of home architecture, development can be described, among other things, in terms of the so-called four generations of retirement homes (Marquardt, 2006). These have continuously evolved with systemic change and the ever-present 'pressure to adapt' from the system and dementia, so that the architecture of a nursing home can also be seen to adapt to changes in the system (cf. Marquardt, 2006).
Conceivable typologies of this quadrant include political systems, possibly also climatic zones (which affect models of nursing home architecture, among others), settlement areas (rural or urban structures, which can also affect nursing home architecture, but also economic aspects of dementia). However, since no evidence can be provided for these factors, typological influences must remain in the hypothetical realm for now.
5.4.3 Internal and external view of dementia in the exterior-collective dimension
Likewise, for the methodologies and theoretical concepts that are mentioned as representative for the inside and outside view of the exterior-collective dimension (cf. ch. 3.2.2.4) of dementia, the limiting remarks of the previous chapters apply to these aspects. In the following, the theory of social autopoiesis will be mentioned as an example for zone 7, the internal view of the exterior-collective dimension of dementia. The term 'systems theory' as representative of zone 8, the external view on the systemic aspects of dementia, is likewise only to be understood as a generic term for a larger number of scientific directions. Figure 23 gives a first impression of the zones of this quadrant and the guiding questions.

Luhmann's theory of social autopoiesis (zone 7) (Kneer & Nassehi, 1993, ch. 3.2.2.4) has not yet been applied to dementia, nor has the theory of Maturana and Varela (1987), on whose approach Luhmann builds. It will be explained here only roughly orienting in a possible relevance for dementia. The theory of social autopoiesis distinguishes between the autopoiesis of, among others, neuronal, mental and social systems (Kneer & Nassehi, 1993, 58), each of which operates separately, i.e. reproduces itself. According to this understanding, human beings are not a single system, but consist of a multitude of closed self-referential systems (Kneer & Nassehi, 1993, 66). The mental as well as the social system are connected to their respective environment by structural coupling, and exchange takes place by means of communication "as last units that cannot be further resolved" (Kneer & Nassehi, 1993, 65).
Assuming that social systems are self-referential systems that reproduce from themselves by means of communication (on Luhmann's concept of communication, cf. Kneer & Nassehi 1993), dementia can possibly be seen as a result of an altered autopoiesis of a consciousness involved in a communication: "A thought appears, but in the very next moment it submerges and is replaced by a new thought. Consciousness thus has to deal with a permanent decay of its elements." (Kneer & Nassehi 1993, 60). Dementia then appears in a basal form in that in this permanent decay of consciousness, individual elements can no longer be reproduced because another structurally coupled system, the neural system, can no longer reproduce certain neural patterns. (Here, however, it must remain open which changes in the structural coupling of the neuronal system may have led to the fact that these patterns are no longer reproduced). Consciousness must now adapt its self-preservation to these changed environmental conditions, which will cause it to change its own structure.
However, since social systems depend on certain environmental conditions for their self-preservation (Kneer & Nassehi, 1993, 69), a altered consciousness directly affects the system as one of these environmental conditions: "Thus, all communication would immediately come to a standstill if at least two consciousness systems were not involved in it." (Kneer & Nassehi, 1993, 69). If a consciousness changes, it thereby provokes or irritates communication as an independent, emergent level of order (Kneer & Nassehi, 1993) of the social system, which then in turn must adapt accordingly in its self-preservation.
The field of systems theory (zone 8), on the other hand, can already draw on multiple data on a relevance of dementia in the system from the external perspective (cf. ch. 3.2.2.4). The results on some lines of the external-collective dimension of dementia mentioned in chapter 5.4.1 can be subsumed under an integral understanding of systems theory that "describes the patterns and interrelations of interactions between external objects (...) from an objective point of view." (Wittrock, 2008, 61). Various aspects of the exterior-collective dimension of dementia mentioned in chapter 5.4.1 and 5.4.2 take on the objective description of the systemic structures that ensure functionality of dementia.
To summarize, here, once again, after chapter 5.2.3, the phenomenon of a heretofore unapplied methodological or theoretical perspective on dementia in zone 7, as opposed to the scientifically well-founded area of zone 8, systems theory with its wide-ranging special references, becomes apparent.
5.5 Summary: Core structures of an integral dementia concept
In the preceding sections, a number of scientific findings about the entity of dementia have been transferred into the structural elements of Integral Theory by way of example. This made it possible to model some structures of an integral dementia concept, focusing on the quadrants and lines of dementia, which are shown together in Figure 24.

Figure 24 clearly shows the four different dimensions of dementia, which originate from the scientific fields and epistemological traditions of the respective quadrants (cf. 3.2.1) and are subject to the validity claim of the respective quadrant (cf. ch. 3.2.1).
The findings about the interior-individual dimension of dementia (cf. ch. 5.1) are subject to the validity claim of truthfulness and give an insight into the interior experience or the subjective perception of what dementia is. The exterior-individual domain, with the scientific domains assigned to it, is subject to the validity claim of truthfulness; the findings of this dimension (cf. ch. 5.2) provide an insight into the various domains of dementia as they can be objectively perceived and described. For the findings of the interior-collective dimension, the claim of justice applies; they show how dementia is perceived, interpreted and integrated in communities (cf. ch. 5.3). Finally, the external-collective dimension of dementia shows how dementia is organized and structured under the validity claim of functional fit (cf. ch. 5.4) in order to maintain its fit in the system.
If we transfer the research data obtained in the preceding sections on the lines of dementia of each quadrant into a quadrant model, a relatively differentiated picture of an integral dementia concept emerges, as figure 25 shows.
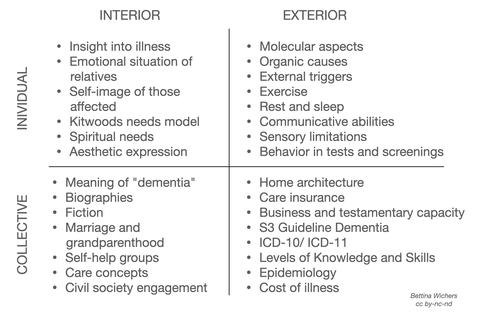
Figure 25 thus shows a detailed subdivision of the entity dementia on the basis of the structural model of the lines, as it has appeared in the literature according to the specifications for the research process mentioned in chapter 4.4. As justified there, this work put the emphasis on the structural models of the quadrants and the lines, while the other aspects were thematized in an overview way.
In summary, according to Figure 25, the aspects of the interior-individual dimension of dementia (cf. ch. 5.1, for all data mentioned in the following section, see references in the respective chapters) are the insight into the disease of both affected persons and, for example, in a modified form of general practitioners, furthermore the emotional situation of relatives, the self-image of affected persons, Kitwood's model of needs, spiritual needs of various persons involved, or the aesthetic self-expression of persons with dementia.
Aspects of the exterior-individual dimension (cf. ch. 5.2) were molecular aspects, different causes of dementia, movement, resting, sleeping and communication as examples of activities of daily living, sensory limitations and the behavior of affected persons in tests and screenings. Here, in contrast to the interior-individual dimension, the focus was exclusively on the perspective of people with dementia, not also other people involved in dementia.
In the interior-collective dimension of the entity dementia (cf. ch. 5.3) data on the (culturally dependent) meaning of the term dementia are available, furthermore biographies of people with dementia, as well as fictional interpretations of the topic. Marriage and grandparenthood under the influence of dementia are assigned to this area according to integral criteria, as are self-help groups, care concepts, or civic engagement.
Aspects of the exterior-collective field of dementia (cf. ch. 5.4) were found in particular in the topics of home architecture and long-term care insurance, but also in the (structural) questions of business and testamentary capacity of people with dementia, in various guidelines such as the S3 guideline on dementia, further development in the field of ICD-10/ ICD-11 or in training structures such as the Scottish Levels of Knowledge and Skills. Finally, findings from epidemiology and on costs of disease complemented this field.
Thus, a detailed picture of a blueprint for an integral dementia concept emerges based on two structural elements of Integral Theory, the quadrants or dimensions and the lines of development. Dementia occurs respectively dementia 'is' (in the sense of a unspecified existence, cf. ch. 4.2) in all these areas of individual as well as collective, inner as well as outer development.
Individual examples for an application of levels, states and types in their relevance for the entity dementia completed the explanations in this chapter. Since they were only exemplary and not detailed, a graphical inclusion is omitted here. An overview of the relevance of the methodologies of the different zones for an integral dementia concept was also presented. Also these are not shown here again, it is referred to the figures 17, 19, 21 and 23.
The main thesis of this paper, that Integral Theory is suitable for the elaboration of a blueprint for an integral dementia concept that can link and integrate wide-ranging findings on the entity of dementia within the conceptual framework, can be considered confirmed according to the data presented here. A blueprint for an integral dementia concept has been presented in this thesis.
The necessary reduction to two structural elements due to the methodological requirements (cf. ch. 4) will be discussed in chapter 7 in terms of its effects on the design and the implications for further research work.
The following chapter 6 is dedicated to the empirical examination of the scope of the presented draft for an integral dementia concept based on a literature analysis.
6 Empirical evaluation of the integral dementia concept
[In chapter 6 there are methodological shortcomings in the sense of circular reasoning, which the reviewers of my work did not criticize, but which I myself consider to be inaccurate
scientific work, which I would like to point out. The imprecision in this chapter was due to the framework conditions, which is an explanation but not an excuse.]
Now that the main thesis of this work has been confirmed in the previous chapter, the related thesis that an integral dementia concept is comprehensive enough to incorporate a wide range of
knowledge about dementia into its structure will be examined (cf. ch. 4.4.2).
In order to obtain a meaningful (but not representative) sample of aspects in the context of dementia, a random sample from the Medline database was chosen as the basis for the empirical review. All titles listed in Medline under the keyword dementia were selected; publications in German from 2011 were chosen as a filter in order to be able to check current data. This resulted in a sample of 45 publications. One dataset was excluded from the content check due to a lack of reference to dementia, leaving 44 datasets. These were categorized according to the topics they focused on using the dimensions of dementia developed in chapter 5 (internal-individual, external-individual, internal-collective, external-collective) with a literature analysis.
6.1 Results of the literature analysis
After analyzing the data sets and evaluating the categories, 11 data sets or publications with a focus on one dimension of dementia (hereinafter referred to as 'one-dimensional'), 22 data sets
with a focus on two dimensions ('two-dimensional') and 11 data sets with a focus on three dimensions ('three-dimensional') were identified. The detailed findings are presented and described
graphically below.
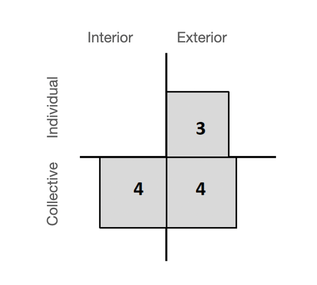
Eleven publications are categorized 'one-dimensionally', i.e. they only focus on topics of a single dimension of dementia according to the integral dementia concept. Figure 26 provides an
overview of the distribution of the one-dimensional publications in the quadrants. While no publication focuses exclusively on the internal-individual area, three publications focus on the
external-individual area, and four each on the internal-collective and external-collective areas of dementia.
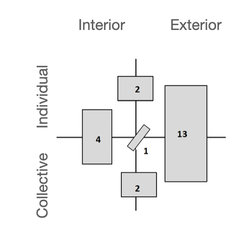
22 of the 44 publications focus on two dimensions of dementia, i.e. indicate a link between two aspects of dementia in the sense of an integral dementia concept. Publications that focus on both the external-individual and the external-collective areas of dementia predominate, with 13 publications compared to a total of nine publications in all other constellations, as Figure 27 shows. Four publications address aspects of the two internal dimensions of dementia, while two publications each focus on combined aspects of the two individual and the two collective dimensions. One publication combines topics of the external-individual and internal-collective areas of dementia (see Fig. 27).
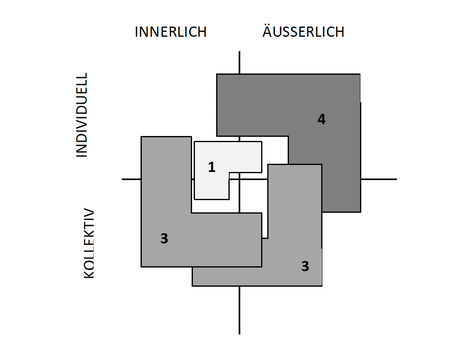
A further eleven publications focus on aspects of three dimensions of dementia, with a relatively balanced distribution (Fig. 28). The informative value of this data is low due to the strong overlaps and the relatively balanced distribution, so this result is not discussed further. However, the data are included in a summarizing evaluation (Fig. 29), as are all the previous ones.
6.2 Summary of the findings
Taking the entire sample together, aspects of the internal-individual dimension were focused on a total of 15 times, the external-individual dimension 26 times, aspects of the internal-collective dimension 19 times and aspects of the external-collective dimension 28 times. Figure 29 provides a graphical overview of the results.

This presentation clearly shows a predominance of the external dimension of dementia with 54 mentions compared to the internal
dimension of dementia with 34 mentions. Furthermore, the collective aspects with 47 thematizations outweigh the internal aspects with 41 mentions. This shows the same tendency in the summary as
in the individual results, i.e. a stronger weighting of the external and collective aspects in the analyzed publications. It is worth mentioning the number of thematizations of aspects of the
internal-individual dimension of dementia, which do not occur as a single topic (see fig. 26) and are therefore only addressed in combination with other aspects of dementia.
Before these results are discussed in detail in the following section, figure 30 shows an overview of the main content of the publications.
If these data are compared with the data in the summary of the integral dementia concept in figure 25, it becomes clear that the findings of the literature study in chapter 5 largely overlap with
the results of the empirical review. The deviations, where they exist, nevertheless show a great deal of similarity in terms of content. A detailed discussion of the findings is provided in the
following section.
6.3 Evaluation
According to the present study, the first thesis of this work (see ch. 4.3) can also be considered confirmed from an empirical point of view: An integral dementia concept, outlined in its main
features in chapter 5, provides the framework to assign all aspects of dementia, represented by a sample of dementia publications in chapter 6, to at least one place in the concept. All data sets
in the sample can be assigned on the basis of the categories of an integral dementia concept, whereby differentiation and assignment according to uni- and multidimensional publications is also
possible.
There is a dominance of the right-sided, external dimension compared to the internal dimension of dementia (54 vs. 34 publications, see fig. 29), but also a predominance of the collective aspects
of dementia compared to the individual aspects of dementia (47 vs. 41 publications, see fig. 29).
The inner-individual area of dementia is the least represented in the publications of the sample used here, which is shown both by the total number of 15 publications focusing on this area (see
fig. 29) and also by the absence of this area in the one-dimensional publications (see fig. 26). The internal-individual aspects do not appear to be the focus of independent consideration in this
sample.
Although the absolute numbers are also only slightly higher compared to the internal-individual area (see fig. 30), the internal-collective area is slightly more represented with 19 publications
and is found in all combination forms, without any particular conspicuous features. However, it is represented in less than half of all publications in the sample.
The external-individual area is the second most frequent topic area with 26 thematizations in the total of 44 publications in the sample, and is found in 50% of them in combination with the
external-collective area alone (see fig. 27).
The external-collective area is the most frequently addressed topic in this sample with 28 thematizations. It is mainly discussed in connection with the external-individual area (see fig.
27).
From this, it can be concluded that the dementia discussion represented in this sample has a greater focus on the external dimension of the dementia entity. Questions about external-collective
structures that make dementia "suitable" (in the sense of the underlying validity claim) for the surrounding system have the highest proportion in this sample. The physical aspects and the
behavior of individuals in connection with dementia are slightly behind as an external-individual dimension.
However, the results of this sample, which are visualized in figures 26 to 29, also show that the second thesis regarding the evidence of a dominance of medicine (see ch. 4.3) cannot be confirmed
on the basis of the purely numerical data. Although it can be concluded from the structures of the dementia concept developed in chapter 5 that the dominance of the external dimensions of
dementia in the sample correlates with a dominance of medical findings, this cannot be deduced from the figures themselves.
However, if we look at the differentiated data situation based on the lines of dementia found in the sample, as shown in figure 30, the following becomes apparent: The exemplary data on, among
other things, pressure sores, wandering behavior and Parkinson's disease (as original fields of activity of medicine, cf. ch. 5.2) in the external-individual dimension, on which the publications
focused, are largely aspects of medical or gerontopsychiatric science. The aspects focused on in the sample, such as medication, guidelines and geriatric psychiatric care structures in the
external-collective dimension of dementia, can largely be assigned to medicine and geriatric psychiatry (cf. ch. 5.4).
The detailed analysis thus provides strong indications of a correlation between the preponderance of data sets from these quadrants and a preponderance of medical findings in these quadrants.
However, as no concrete distributions were collected here, no clear evidence can be provided for this thesis. In a further analysis, it would be necessary to work out the categories in a more
differentiated way using the lines, levels, states and typologies of the integral dementia concept and to re-examine the sample. However, this is not done here, as the confirmation of the first
thesis and strong evidence against a rejection of the second thesis are considered sufficient results.
7 Integral Theory as the Basis for an Integral Dementia Concept. Concluding Discussion
The aim of this thesis was to create a blueprint for an integral dementia concept based on the structural models (cf. ch. 3.1) and the concept of Integral Methodological Pluralism (cf. ch. 3.2.3) of Integral Theory. This outline could be derived in chapter 5 using data from dementia research and other areas of knowledge about dementia. Chapter 5.5 shows a graphical representation of the design based on the superordinate lines (fig. 24) and on the detailed data in the individual dimensions of dementia (fig. 25).
In chapter 6, the thesis that an integral dementia concept is suitable for integrating and linking data from a broad spectrum of knowledge about dementia was empirically tested. On the basis of a literature analysis of scientific publications on dementia, it was shown that all the data sets could be assigned to at least one dimension of dementia (cf. ch. 6.1), as shown in the draft of an integral dementia concept (cf. ch. 5). Furthermore, the data showed that the draft could be used to visualize the dominance of medical issues in the scientific discussion represented here (cf. ch. 6.3).
Thus, according to the findings presented here, Integral Theory provides the appropriate framework to represent the entity of dementia in its multidimensionality. An integral dementia concept thus eliminates the perspective viewpoint adopted by some dementia concepts. The draft presented here shows that a wide-ranging picture of dementia can emerge by bringing together different epistemological traditions and scientific fields (cf. ch. 5.5). This allows to see dementia from several perspectives at the same time and shows for all perspectives the fundamental same recognition as a relevant contribution to a holistic picture of dementia.
Furthermore, the design of an integral dementia concept offers the opportunity to present key findings in the current scientific discussion on dementia. In the current research literature reviewed here, a dominance of external aspects of dementia could be shown and visualized using the quadrant model (see figs. 26 - 29). In the detailed analysis of the aspects of dementia focused on by the research literature, a dominance of medical aspects was demonstrated (cf. ch. 6.3).
Various aspects of an integral dementia concept were only hinted at in this thesis in their potential for further integral dementia research. The structural elements of levels, states and typologies, which were only reviewed in overview due to the necessary methodological limitations (cf. ch. 4), and the different zones of Integral Methodological Pluralism (cf. ch. 3.2.2) showed points of contact for further insights into dementia from an integral perspective.
The challenge formulated in chapter 4, to describe a phenomenon of consciousness that includes regression on the basis of a theoretical theory oriented toward forward or upward development, was met by the outline for an integral dementia concept, but the specific topic was not captured in detail by the methodology used. It will be the task of further research to investigate the interrelationships between different developmental directions, in particular through the increased use of level models.
In this context, understanding of medications as states in the exterior-individual realm should also be pointed out once again, which takes an unusual look at medicinal therapeutics and especially at the intensive research behind them: In this outline for an integral dementia concept, medications occupy a rather marginal place; they are understood as artifacts of the exterior-collective quadrant (cf. ch. 5.4.1) and as such induce alterations of states in specific lines of the exterior-individual quadrant (cf. ch. 5.2.2). This perspective on pharmacological therapeutics does not devalue pharmaceutical research and its 'artifacts', but it does relativize their status - at least from an integral point of view.
Here the potential of an integral dementia concept to be deepened with an extended methodology becomes apparent: it should go into depth on the many individual aspects of dementia as already shown in this draft, research further aspects, describe different levels in detail in the different lineages, question the influences of different conditions and consider in detail the influence of typologies on the aspects mentioned so far. It is also necessary to show connections between the different dimensions, lines and levels and to try to find them where no connections can be found so far.
A comprehensive integral dementia concept may be able to show how the lines and levels of the dimensions of dementia are interwoven and could serve as a frame of reference for practitioners as well as theorists with respect to their own standpoint in the fabric of the entity of dementia as well as with respect to other standpoints, insights, and techniques. The outline of an integral dementia concept presented here shows approaches to this.
Bibliography
Internet resources were rechecked on 04/23/2023; pages still available online are noted with that date. For all other
pages that are no longer online, the date of the last review in September 2011 is indicated. Titles of German sources itself are translated; where original English sources were available, these
were given first before the German title.
Aktion Demenz (n.d. a). Gemeinsam für ein besseres Leben mit Demenz. [Together for a better life with dementia]. http://www.aktion-demenz.de [08.02.2024].
Aktion Demenz (n.d. b). Aufruf: In unserer Kommune - gemeinsam für ein besseres Leben mit Demenz. [Call: In our community - together for a better life with dementia.] http://www.aktion-demenz.de/images/stories/pdf/Aufruf.pdf [08.02.2024].
Arp, A. (2011). Wir tanzen wieder – Demenz und Bewegung. [We are dancing again - dementia and movement.] ProAlter, 2, 9-11.
Bachl, M. (2011). Den Würdebegriff täglich mit Inhalt füllen. [Filling the concept of dignity with content on a daily basis.] Krankenpflege [Schweiz], 104 (1), 19-21.
Bachl, M. (2011). Licht in dunkle Seelenlandschaft bringen. [Shedding light on dark landscapes of the soul.] Krankenpflege [Schweiz], 104 (5), 18-19.
Balikci, A. (in press). Kultursensible Altenarbeit bei Migranten mit Demenz. Das Herz vergisst nicht. [Culturally sensitive eldercare in migrants with dementia. The heart does not forget.] Pflegezeitschrift, 64 (8), 464-467.
Ballenger, J. F. (2006). Self, Senility, and Alzheimer’s Disease in Modern America. A History. Baltimore: The John Hopkins University Press.
Banzhaf, M., Klarl, B. A.& Braun, B. (2011). Demenz bei Morbus Whipple? Die Bedeutung infektiöser Krankheitsursachen. [Dementia in Whipple's disease? The importance of infectious causes of disease.] Deutsche medizinische Wochenschrift, 136 (24), 1312-1315.
Bauer, A. M. (2011). Kachektischer AIDS-Patient mit Soor, Gastritis, Kolitis, Tremor, Nierenversagen… Nach 13 Jahren war die Grenze der Polypharmazie erreicht. [Cachectic AIDS patient with thrush, gastritis, colitis, tremor, kidney failure... After 13 years, the limit of polypharmacy was reached.] MMW Fortschritte der Medizin, 135 (18), 45-46.
Becker, S., Kruse, A., Schröder, J. & Seidl, U. (2005). Das Heidelberger Instrument zur Erfassung von Lebensqualität bei Demenz (H.I.L.D.E.). Dimensionen von Lebensqualität und deren Operationalisierung. [The Heidelberg Instrument for the Assessment of Quality of Life in Dementia (H.I.L.D.E.). Dimensions of quality of life and their operationalization.] Zeitschrift für Gerontologie und Geriatrie, 38, 108-121.
Belschner, W. (2010). Forschen, erfahrungsbasiert. Eine bewusstseinspsychologische Perspektive. [Research, experience based. A perspective of consciousness psychology.] Kröning: Asanger-Verlag.
Benkert, O., Hautzinger, M. & Graf-Morgenstern, M. (2007). Psychopharmakologischer Leitfaden für Psychologen und Psychotherapeuten. [Psychopharmacological guide for psychologists and psychotherapists.] Heidelberg: Springer Medizin Verlag.
Berendonk, C., Stanek, S., Schönit, M., Kaspar, R., Bär, M. & Kruse, A. (2011). Biographiearbeit in der stationären Langzeitpflege von Menschen mit Demenz: Potenziale des DEMIAN-Pflegekonzepts. [Biography work in inpatient long-term care of people with dementia: potentials of the DEMIAN care concept.] Zeitschrift für Gerontologie und Geriatrie, 44 (1), 13-18.
Bornemann-Cimenti, H., Wejbora, M., Michaeli, K., Kern-Pirsch, C., Sandner-Kiesling, A. (2011). Schmerzerfassung bei Demenz. [Pain assessment in dementia.] Der Nervenarzt 82 (9), 1-6.
Braun, S. & Kriegeskorte, P. (2011). Ehrenamtliche sorgen für bunte Abwechslung. Aktivierende Gruppenbetreuung für demenzkranke Patienten. [Volunteers provide colorful variety. Activating group care for patients with dementia] Pflegezeitschrift, 64 (2), 86-88.
Bundesministerium für Familie, Senioren, Frauen und Jugend [Federal Ministry for Family Affairs, Senior Citizens, Women and Youth] [BMFSFJ] (o.J.): Demenzerkrankung – eine Einführung. [Dementia - an introduction]. http://www.wegweiser-demenz.de/ demenzerkrankung.html [26.08.2011].
Bundesministerium der Justiz [Federal Ministry of Justice] [BMJ] (2009): Gesetz über die Berufe in der Altenpflege [Law on professions in geriatric care] (Altenpflegegesetz - AltPflG). [Zuletzt geändert durch Art. 12b G v. 17.7.2009]. http://www.gesetze-im-internet.de/bundesrecht/altpflg/gesamt.pdf [16.09.2011].
Bundesministerium der Justiz [Federal Ministry of Justice] [BMJ] (2011a). Sozialgesetzbuch [Social Code] (SGB) Fünftes Buch (V) – Gesetzliche Krankenversicherung - (Artikel 1 des Gesetzes v. 20. Dezember 1988, BGBl. I S. 2477). [Zuletzt geändert durch Art. 3 G v. 28.7.2011]. http://www.gesetze-im-internet.de/bundesrecht/sgb_5/gesamt.pdf [08.02.2024].
Bundesministerium der Justiz [Federal Ministry of Justice] [BMJ] (2011b). Sozialgesetzbuch [Social Code] (SGB) - Elftes Buch (XI) - Soziale Pflegeversicherung. [Zuletzt geändert durch Art. 6 G v. 28.7.2011]. http://www.gesetze-im-internet.de/sgb_11/ BJNR101500994.html [11.04.2023].
Dammann, R. & Gronemeyer, R. (2009). Ist Altern eine Krankheit? Wie wir die gesellschaftlichen Herausforderungen der Demenz bewältigen. [Is aging a disease? How we cope with the societal challenges of dementia.] Frankfurt a.M.: Campus-Verlag.
Demenz Support Stuttgart (Hrsg.) (2010a): Philosophie. [Philosophy]. http://www.demenz-support.de/portraet/philosophie [01.09.2011].
Demenz Support Stuttgart (2010b): Ich spreche für mich selbst. [I speak for myself]. http://www.demenz-support.de/arbeitsfelder/teilhabe_und_gesellschaft/ ich_spreche_fuer_mich_selbst. [01.09.2011].
Deutsche Alzheimer Gesellschaft [German Alzheimer Society] (2008): Was heißt eigentlich „Demenz“ und „Alzheimer“? [What does "dementia" and "Alzheimer's" actually mean?]. http://www.deutsche-alzheimer.de/index.php?id=25 [26.08.2011].
Deutsche Gesellschaft für Psychiatrie, Psychotherapie und Nervenheilkunde und Deutsche Gesellschaft für Neurologie [DGPPN & DGN] (Hrsg.) (2009). S3-Leitlinie „Demenzen“ (Kurzversion). [S3 guideline "Dementias" (short version).] http://www.dgn.org/images/stories/dgn/leitlinien /ll_demenz/ll-demenz-kurz-170210.pdf [23.06.2011].
Deutscher Ethikrat [German Ethics Council] (2010). Podiumsdiskussion. [Panel discussion] [Audio transcript]. Deutsche Ethikkommission: Demenz – Ende der Selbstbestimmung? Öffentliche Tagung, 24.11.2010. [German Ethics Committee: dementia - end of self-determination? Public Conference] Hamburg. http://www.ethikrat.org/veranstaltungen/weitere-veranstaltungen /demenz-ende-der-selbstbestimmung [27.08.2011].
Deutscher Wortschatz (2011). Konzept. [Concept]. Universität Leipzig. http://wortschatz.uni-leipzig.de/ [28.09.2011]
Deutsches Institut für Medizinische Dokumentation und Information [DIMDI] (2010). ICD-10-WHO Version 2011. Kapitel V Psychische und Verhaltensstörungen (F00-F99). Organische, einschließlich symptomatischer psychischer Störungen (F00-F09). [ICD-10-WHO version 2011. chapter V Mental and behavioral disorders (F00-F99). Organic, including symptomatic mental disorders (F00-F09).] http://www.dimdi.de/static/de/klassi/diagnosen/icd10/htmlamtl/fr-icd.htm?gf00.htm+ [13.09.2011].
Drach, L. M. (2011). Pharmakotherapie bei Demenz mit Lewy-Körperchen und Parkinson-Demenz. Gemeinsamkeiten und Unterschiede. [Pharmacotherapy in dementia with Lewy bodies and Parkinson's dementia. Similarities and differences.] Medizinische Monatsschrift für Pharmazeuten, 34 (2), 47-52.
Egidi, G. (2011). Verbesserte ambulante Demenzversorgung. [Kommentar]. [Improving outpatient dementia care. Commentary]. Deutsche medizinische Wochenschrift 136 (28-29), 1493.
Engel, S. (2006). Alzheimer und Demenzen. Unterstützung für Angehörige. Die Beziehung erhalten mit dem neuen Konzept der einfühlsamen Kommunikation. [Alzheimer's disease and dementias. Support for family members. Preserving the relationship with the new concept of empathetic communication.] Stuttgart: Trias.
Engel, S. (2007). Belastungserleben bei Angehörigen Demenzkranker aufgrund von Kommunikationsstörungen. [Experiencing stress in relatives of dementia patients due to communication disorders.] Münster: LIT Verlag.
Engel, S. (2008). Angehörigenberatung – Verbesserung der Situation pflegender Angehöriger als ein zentrales Arbeitsfeld der Gerontopsychiatrie. [Counseling of relatives - Improving the situation of caring relatives as a central field of work in gerontopsychiatry.] In: W.D. Oswald, G. Gatterer & U.M. Fleischmann (Hrsg.), Gerontopsychologie. Grundlagen und klinische Aspekte zur Psychologie des Alterns. Wien, New York: Springer, 2. Auflage. 195-212.
Engel, S.; Mück, A., Lang, F.R. (2009). Kognitives Screening. [Cognitive Screening]. In: R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 122-131.
Engel, S. (2011). Multiperspektivische Betrachtung der Demenz. [Multiperspective view of dementia.] [Vorlesungsskript]. Erlangen: Institut für Psychogerontologie.
Esbjörn-Hargens, S. (2009). An overview of Integral Theory: An all-inclusive framework for the twenty-first century. [Eine Übersicht integraler Theorie. Ein allumfassendes Bezugssystem für das 21. Jahrhundert. http://if.integralesforum.org/fileadmin/ user_upload/LESESAAL/PDF/Integrale_Theorie_-_S._Esbjoern-Hargens.pdf [10.08.2011].] Original: https://integralwithoutborders.org/sites/default/files/resources/Intro_Integral_Theory.pdf [08.02.2024].
Feil, N. (1992). Validation. Ein neuer Weg zum Verständnis alter Menschen. [Validation. A new way to understand the elderly.] Wien: Altern und Kultur.
Fischer, T., Worch, A., Nordheim, J., Hasselhorn, H. M., Wulff, I. M., Gräske, J., Meye, S. & Wolf-Ostermann, K. (2011). Ambulant betreute Wohngemeinschaften für alte, pflegebedürftige Menschen – Merkmale, Entwicklung und Einflussfaktoren. [Outpatient assisted living communities for elderly people in need of care - Characteristics, development and influencing factors.] Pflege, 24 (2), 97-109.
Franke, L. (2005). Demenz in der Ehe : über die verwirrende Gleichzeitigkeit von Ehe- und Pflegebeziehung in der psychosozialen Beratung für Ehepartner Demenzkranker. [Dementia in marriage: on the confusing simultaneity of marital and caregiving relationships in psychosocial counseling for spouses of dementia patients.] [Dissertation]. Bielefeld: Universität Bielefeld. https://pub.uni-bielefeld.de/luur/download?func=downloadFile&recordOId=2304578&fileOId=2304583 [30.08.2011]
Förstl, H. (2009a) (Hrsg.). Demenzen in Theorie und Praxis. [Dementias in theory and practice.] Heidelberg: Springer Medizin Verlag. 2. Auflage.
Förstl, H. (2009b). Was ist Demenz. [What is dementia.] In: H. Förstl (Hrsg.), Demenzen in Theorie und Praxis. Heidelberg: Springer Medizin Verlag. 2. Auflage. 4-7.
Fuhr, R. & Gremmler-Fuhr, M. (2004). Kommunikationsentwicklung und Konfliktklärung. Ein integraler Gestalt-Ansatz. [Communication development and conflict resolution. An integral Gestalt approach.] Göttingen: Hogrefe.
Geiger, A. (2011). Der alte König in seinem Exil. [The old king in his exile.] München: Carl Hanser Verlag.
Gemsenjäger, E. (2011). Sind Ethikfachleute im chirurgischen Alltag notwendig? [Are ethics professionals necessary in everyday surgery?] Der Chirurg, 82 (19), 80.
GKV - Spitzenverband der Pflegekassen [GKV] (2008). Richtlinien nach § 87b Abs. 3 SGB XI zur Qualifikation und zu den Aufgaben von zusätzlichen Betreuungskräften in Pflegeheimen [Guidelines according to § 87b Abs. 3 SGB XI on the qualification and tasks of additional caregivers in nursing homes] (Betreuungskräfte-Rl vom 19. August 2008). https://www.gkv-spitzenverband.de/upload/2008_08_19__%C2%A787b_Richtlinie_2291.pdf [16.09.2011].
Gogol, M. (2011). Medien: Diagnose und Behandlungsleitlinie Demenz. [Rezension]. [Media: diagnosis and treatment guideline dementia. Review]. Zeitschrift für Gerontologie und Geriatrie, 44 (1), 71.
Gräßel, E., Stemmer, R., Abt, S. M., Eichenseer, B. & Luttenberger, K. (2011). Zweifel ausgeräumt. [Doubts dispelled.] Pflegezeitschrift 64 (4), 201-204.
Groll, A. E. (2008). Geschlechtsspezifische Unterschiede in der ambulanten Versorgung von Demenzpatienten. Sekundäranalyse einer postalischen Befragung zur Versorgungssituation von Patienten mit kognitiven Beeinträchtigungen und Demenzen. [Gender differences in outpatient care of dementia patients. Secondary analysis of a postal survey on the care situation of patients with cognitive impairment and dementia.] [Dissertation]. Universität Hamburg. [New ressource:] https://ediss.sub.uni-hamburg.de/handle/ediss/2531 [08.02.2024].
Grond, E. (1997). Altenpflege als Beziehungspflege. Ein interaktionelles Pflegekonzept. [Elderly care as relational care. An interactional concept of care.] Hagen: Brigitte Kunz Verlag.
Haass, C. (2006). Alzheimer – das molekulare Uhrwerk einer tickenden Zeitbombe. [Alzheimer's disease - the molecular clockwork of a ticking time bomb.] In Nationaler Ethikrat (Hrsg.), Altersdemenz und Morbus Alzheimer. Medizinische, gesellschaftliche und ethische Herausforderungen. Vorträge der Jahrestagung des Nationalen Ethikrates 2005. Berlin: Nationaler Ethikrat. 19-26.
Habecker, M. (2010). Typen. [Types] [Text zusammengestellt von M. Habecker]. Integral informiert, 23, 7-24.
Hanns, S., Born, A., Nickel, W. & Brähler, E. (2011). Versorgungsstrukturen in stationären Pflegeeinrichtungen: Eine Untersuchung in Leipziger Pflegeheimen. [Care structures in inpatient nursing homes: An investigation in Leipzig nursing homes.] Zeitschrift für Gerontologie und Geriatrie, 44 (1), 33-38.
Heinemeyer, C. (2011). Diskussion um Demenz-Pflege. [Discussion on dementia care.] [Editorial]. Pflegezeitschrift, 64 (1).
Heinemeyer, C. (2011). Planvoll managen und trotzdem Raum für Versuch und Irrtum lassen. [Managing according to plan while still leaving room for trial and error.] [Editorial]. Pflegezeitschrift 64 (6), 321.
Hessenauer, A. (o.J.). Apoptosemechanismen und neurodegenerative Erkrankungen. Die Alzheimer-Demenz. Apoptosis mechanisms and neurodegenerative diseases. Alzheimer's disease. [Power-Point-Präsentation]. http://wwwalt.med-rz.uni-sb.de /med_fak/biochemie/ApoAlz.pdf [09.09.2011].
Höft, B., Sadeghi-Seradi, A., List, M. &Supprian, T. (2011). Die Einbindung von Menschen mit Demenz und fehlendem Krankheitserleben in ein ambulantes Hilfesystem durch gerontopsychiatrische Hausbesuche. [Engaging people with dementia and missing illness experience in an outpatient support system through gerontological psychiatric home visits.] Psychiatrische Praxis, 38 (4), 198-200.
Höwler, E. (2008). Herausforderndes Verhalten bei Menschen mit Demenz. Erleben und Strategien Pflegender. [Challenging behavior in people with dementia. Experiences and strategies of caregivers.] Stuttgart: Kohlhammer.
Holthoff, V. (2009). Klassische Bildgebung. [Classical imaging.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 141-146.
Integral Research Center (2009). References of M.A. Theses & Ph.D. Dissertations Using Integral Theory. http://www.integralresearchcenter.org/sites/default/files/Dissertations-Theses.pdf [31.05.2011].
Jens, T. (2009). Demenz. Abschied von meinem Vater. [Dementia. Farewell to my father.] Gütersloh: Gütersloher Verlagshaus.
Jessen, F. (2009a). Liquordiagnostik. [CSF diagnostics.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 152-156.
Jessen, F. (2009b). Genetik. [Genetics.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 156-160.
Jonas, I. (2006). Kinder- und Jugendliteratur zu Demenz. [Children's and adolescent literature on dementia.] ProAlter, 3, 56-58.
Jonas, I. (2008). Doppelt ausgeschlossen: Menschen mit Demenz und Hörschädigung. [Doubly excluded: People with dementia and hearing impairment.] ProAlter, 3, 33-36.
Jonas, I. (2009). "Hier kriegt mich keiner mehr weg!". Menschen mit Demenz erleben Kunst im Museum. ["Nobody can get me out of here!". People with dementia experience art in museums.] ProAlter 4, 51-54.
Jürgs, M. (2001): Alzheimer. Spurensuche im Niemandsland. [Alzheimer's disease. Searching for traces in no man's land.] München: List Taschenbuch Verlag.
Kastner, U. & Löbach, R. (2007). Handbuch Demenz. [Dementia handbook.] München: Urban & Fischer.
Kaufmann, E. (2010). Subjektives Wohlbefinden von Menschen mit Demenz – eine qualitative Interviewstudie auf der Basis des Bedürfnismodells von Tom Kitwood. [Subjective well-being of people with dementia - a qualitative interview study based on Tom Kitwood's needs model.] [Unveröffentlichte Masterarbeit]. Erlangen: Institut für Psychogerontologie.
Kieckebusch, U. von (2010). Psychologische Demenzdiagnostik. [Psychological dementia diagnostics.] München: Ernst Reinhardt.
Kiencke, P.; Rychlik, R.; Grimm C. & Daniel, D. (2010). Krankheitskosten bei Alzheimer-Demenz. [Cost of illness in Alzheimer's disease.] Medizinische Klinik 105, 327-333.
Kneer, G. & Nassehi, A. (1993). Niklas Luhmanns Theorie sozialer Systeme. Eine Einführung. [Niklas Luhmann's social systems theory. An introduction.] München: Fink
König, R. (2009). Wissenschaft in Wikipedia und anderen Wikimedia-Projekten. [Science in Wikipedia and other Wikimedia projects.] ITA-Projektbericht Nr.: A52-2. Wien, Institut für Technikfolgen-Abschätzung (ITA). http://epub.oeaw.ac.at/ita/ita-projektberichte/d2-2a52-2.pdf [08.02.2024].
Köther, I., Gnamm, E. (1995). Altenpflege in Ausbildung und Praxis. [Geriatric nursing in education and practice. ]Stuttgart: Thieme Verlag.
Komarahadi, F. L., Ruf, D., Hüll, M. & Härter, M. (in Druck). Informationsbedarf von Ärzten, Pflegepersonal und Angehörigen für eine evidenzbasierte Internetseite zum Thema Demenz. [Information needs of physicians, nurses, and family members for an evidence-based website on dementia. Psychiatric Practice] Psychiatrische Praxis. https://www.thieme-connect.de/ejournals /pdf/psychiat-praxis/doi/10.1055/s-0031-1276837.pdf [27.09.2011].
Kompetenznetz Demenzen (o.J.): Wissenswertes über Demenzen. [Facts worth knowing about dementia.] http://www.kompetenznetz-demenzen.de/betroffene/ wissenswertes/ [27.08.2011].
Kreutzner, G. (2008). Demenz und Kultur: Zwei Perspektiven. [Dementia and culture: two perspectives]. DeSSorientiert, 1. Stuttgart: Demenz Support Stuttgart. 6-16. http://www.demenz-support.de/Repository/dess journal_1_1_2009_hearing2.pdf [01.09.2011].
Kruse, A. (2010). Die Lebensqualität demenzkranker Menschen erfassen und positiv beeinflussen – eine fachliche und ethische Herausforderung. [Capturing and positively influencing the quality of life of people with dementia - a professional and ethical challenge.] [Audio protocol]. Deutsche Ethikkommission: Demenz – Ende der Selbstbestimmung? Öffentliche Tagung, 24.11.2010. Hamburg. http://www.ethikrat.org/veranstaltungen/weitere-veranstaltungen/demenz-ende-der-selbstbestimmung [08.02.2024].
Küpers, W. (2006). Integrales Lernen in und von Organisationen. [Integral learning in and of organizations.] Integral Review 2, 43-77. New Ressource: https://integral-review.org/integrales-lernen-in-und-von-organisationen/ [08.02.2024].
Küstenmacher, M., Haberer, T. & Küstenmacher, W. T. (2011). Gott 9.0. Wohin unsere Gesellschaft spirituell wachsen will. [God 9.0. Where our society wants to grow spiritually.] Gütersloh: Gütersloher Verlagshaus, 2. Auflage.
Kurz, A. & Wilz, G. (2011). Die Belastung pflegender Angehöriger bei Demenz: Entstehungsbedingungen und Interventionsmöglichkeiten. [The burden of caring relatives in dementia: conditions of emergence and possibilities for intervention.] Der Nervenarzt, 82 (3), 336-342.
Land Hessen [State of Hesse] (2007). Hessisches Gesetz über die Ausbildung in der Altenpflegehilfe und zur Ausführung des Altenpflegegesetzes (Hessisches Altenpflegegesetz – HaltPflG) [Hessian Law on Training in Elderly Care Assistance and Implementation of the Elderly Care Act (Hessian Elderly Care Act] vom 05.Juli 2007. http://www.landesrecht-hessen.de/hessenrecht/353_Heilhilfsberufe_ Hebammen/353-56-HAltPflG/HAltPflG.htm#%C2%A7_27 [16.09.2011].
Laske, C. (2007). Was schützt vor Demenz? Auf der Suche nach dem geistigen Jungbrunnen. [What protects against dementia? In search of the mental fountain of youth.] Zeitschrift für Gerontopsychologie & -psychiatrie, 20 (1), 59-67.
Lauter, H. (2011). Ärztliche Suizidassistenz bei Demenzerkrankungen? [Physician assisted suicide in dementia?] Der Nervenarzt, 82 (1), 50-56.
Lempert, T. & Bschor, T. (2011). Behandlung des M. Alzheimer nach der S3-Leitlinie Demenzen. Cholinesteraseinhibitoren für alle und für immer? [Kommentar] [Treatment of Alzheimer's disease according to the S3 guideline Dementias. Cholinesterase inhibitors for all and forever? Commentary]. Der Nervenarzt, 82 (1), 90-91
Lichtenwimmer, A. (2010). Geschäfts- und Testierfähigkeit in der Praxis des Notars. [Business and testamentary capacity in notary practice.] In M. Schmoeckel (Hrsg). Demenz und Recht. Bestimmung der Geschäfts- und Testierfähigkeit. Baden-Baden: Nomos. 43-56.
Lind, S. (2000). Umgang mit Demenz. Wissenschaftliche Grundlagen und praktische Methoden. Ergebnisse einer Literaturrecherche und Sekundäranalyse der Fachliteratur in internationalen Pflegezeitschriften zur psychogeriatrischen Pflege und Betreuung Demenzkranker. [Dealing with dementia. Scientific foundations and practical methods. Results of a literature search and secondary analysis of the literature in international nursing journals on psychogeriatric nursing and care of dementia patients.] Stuttgart: Paul-Lempp-Stiftung. http://www.gerontologische-beratung-haan.de/dokumente/ Wissen24LemppA.pdf [20.09.2011].
Lind, S. (2011). Replik auf die Leserbriefe von Christian Müller-Hergl und Michael Thomsen. [Kommentar]. Das Missverständnis. [Replica to the letters to the editor by Christian Müller-Hergl and Michael Thomsen. [Commentary]. The misunderstanding.] Pflegezeitschrift, 64 (3), 134-136.
Luppa, M., Gentzsch, K., Angermeyer, M. C., Weyerer, S., König. H. H. & Riedel-Heller, S. (2011). Geschlechtsspezifische Prädiktoren von Institutionalisierung im Alter - Ergebnisse der Leipziger Längsschnittstudie in der Altenbevölkerung [Gender-specific predictors of institutionalization in old age - Results from the Leipzig Longitudinal Study in the Elderly Population] (Leila 75 +). Psychiatrische Praxis, 38 (4), 185-189.
Mahlberg, R. (2009). Schlafstörungen. [Sleep disorders.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 104-108.
Mahlberg, R. & Gutzmann, H. (2009a). Demenzerkrankungen erkennen, behandeln und versorgen. [Recognizing, treating, and caring for dementia.] Köln: Deutscher Ärzte-Verlag.
Mahlberg, R.& Gutzmann, H. (2009b). Einleitung: Krankheitsbilder. [Introduction: Clinical pictures.] In R. Mahlberg & Gutzmann, H. (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 3-10.
Mahlberg, R. & Kunz, D. (2009). Zirkadiane Rhythmusstörungen. [Circadian rhythm disorders.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 216-221.
Marpert, M., Roser, M. (2011). Gedächtnissprechstunden in der gemeindepsychiatrischen Versorgung. [Memory consultations in community psychiatric care.] Psychiatrische Praxis 38 (4), 163-165.
Marquardt, G. (2006). Kriterienkatalog Demenzfreundliche Architektur. Möglichkeiten zur Unterstützung der räumlichen Orientierung in stationären Altenpflegeeinrichtungen. [Criteria catalog dementia-friendly architecture. Possibilities to support spatial orientation in inpatient geriatric care facilities.] [Dissertation]. Dresden: Technische Universität Dresden. http://deposit.d-nb.de/cgi-bin/dokserv?idn=985850043 &dok_var=d1&dok_ext=pdf&filename=985850043.pdf [20.09.2011].
Maturana, H. R. & Varela, F. J. (1987). Der Baum der Erkenntnis. [The tree of knowledge.] Goldmann-Verlag.
McFarlane, T. J. (2000). A Critical Look at Ken Wilber’s Four Quadrant Model. http://www.integralscience.org/wilber.html [11.04.2023].
McIntosh, S. (2007) Integral consciousness and the future of evolution. How the integral worldview is transforming politics, culture, and spirituality. [German: Integrales Bewusstsein und die Zukunft der Evolution. Wie die integrale Weltsicht Politik, Kultur und Spiritualität transformiert. (2009) Hamburg: Phänomen-Verlag.]
Meyerhoff, J. (2006): Six Criticisms of Wilber's Integral Theory. http://www.integralworld.net/meyerhoff4.html [08.02.2024].
Meyers Großes Taschenlexikon (1992). Konzept. [Concept.] [24 Bände]. Mannheim: BI Taschenbuchverlag.
Michel, C. & Niemann, A. (2002). Sozioökonomische Bedeutung der Demenz und leichter kognitiver Störungen. [Socioeconomic significance of dementia and mild cognitive impairment.] Versicherungsmedizin, 54, 1, 26-32.
Miller, T. (1999). Systemtheorie und Soziale Arbeit. Ein Lehr- und Arbeitsbuch. [Systems theory and social work. A textbook and workbook.] Stuttgart: Enke
Müller, K. (2008). Prävention: Wer rastet, der rostet – Bewegung wirkt präventiv gegen Demenz. [Prevention: a rolling stone gathers no moss - exercise has a preventive effect against dementia.] DeSSorientiert, 2, 16-22. Stuttgart: Demenz Support Stuttgart. http://www.demenz-support.de/Repository/dessjournal_2_2008_ bewegung.pdf [09.09.2011].
Müller-Hergl, C. (2007). Menschen mit Demenz: Spirituelle Bedürfnisse. [People with dementia: spiritual needs.] DeSSorientiert, 2, 23-27. Stuttgart: Demenz Support Stuttgart. http://www.demenz-support.de/ Repository/dessjournal_2_2007_ spiritualitaet.pdf [08.09.2011].
Müller-Hergl, C. (2011). „Die Welt des Herrn Lind beruht auf Fehlschlüssen.“ [Kommentar]. ["Mr. Lind's world is based on fallacies." Commentary]. Pflegezeitschrift 64 (1), 6-8.
Myllymäki-Neuhoff, J. (2009). Wohn- und Betreuungsformen. [Residential and assisted living arrangements.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 261-271.
Natale, B., Wohrab, D., Förtsch, B., Kurz, A. & Diehl-Schmid, J. (2011). Die Alzheimer-Demenz mit senilem Beginn - Besonderheiten in Diagnostik, Therapie und Management. [Alzheimer's disease with senile onset - special features in diagnosis, therapy and management.] Fortschritte der Neurologie – Psychiatrie, 79 (3), 144-151.
Nentwich, M. (2009). Cyberscience 2.0 oder 1.2? Das Web 2.0 und die Wissenschaft. [Cyberscience 2.0 or 1.2? Web 2.0 and science.] ITA-manuscripts 11. Wien, Institut für Technikfolgen-Abschätzung (ITA). http://www.oeaw.ac.at/ita/ita-manus.htm [01.10.2011].
Neumann, E.-M. (2009). Exkurs 2: Geschlechtsrollenunterschiede. [Excursus 2: Gender role differences.] In R. Mahlberg & H. Gutzmann (Hrsg.): Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 285-290.
Nocon, M., Roll, S., Schwarzbach, C., Vauth, C., Greiner, W. & Willich, S.N. (2010). Pflegerische Betreuungskonzepte bei Patienten mit Demenz. Ein systematischer Review. [Nursing care concepts in patients with dementia. A systematic review.] Zeitschrift für Gerontologie und Geriatrie, 43 (3), 183-189.
Nufer, T. W. & Spichiger, E. (in Druck). Wie Angehörige von Patientinnen mit Demenz deren Aufenthalt auf einer Akutstation und ihre eigene Zusammenarbeit mit Fachpersonen erleben. Eine qualitative Studie. [How relatives of patients with dementia experience their stay in an acute care unit and their own collaboration with professionals. A qualitative study.] Pflege, 24 (4), 229-237.
Palmer, H. (1991). Das Enneagramm. Sich selbst und andere verstehen lernen. [The Enneagram. Learning to understand oneself and others.] München: Knaur.
Pentzek, M., Fuchs, A. & Abholz, H.H. (2005). Die Einstellung der Hausärzte zu Demenzen. Kognitivem affektive und externe Komponenten. [General practitioners' attitudes toward dementia. Cognitive affective and external components.] Nervenheilkunde, 24, 499-506.
Perneczky, R., Alexopoulos, P., Schmid, G, Sorg, C., Förstl, H., Diehl-Schmid, J. & Kurz, A. (2011). Kognitive Reservekapazität und ihre Bedeutung für Auftreten und Verlauf der Demenz. [Cognitive reserve capacity and its relevance for dementia onset and progression.] Der Nervenarzt, 82 (3), 325-335.
Pfeifer-Schaupp, U. (2009). Prä-Therapie in der Altenpflege. Neue Zugänge zu Menschen mit schwerer Demenz. [Pre-therapy in geriatric care. New approaches to people with severe dementia.] Zeitschrift für Gerontologie und Geriatrie, 42 (4), 336-341.
Philipp-Metzen, H. E. (2008). Die Enkelgeneration im ambulanten Pflegesetting bei Demenz. Ergebnisse einer lebensweltorientierten Studie. [The grandchild generation in dementia outpatient care settings. Results of a lifeworld-oriented study.] Wiesbaden: Verlag für Sozialwissenschaften.
Philipp-Metzen, H. E. (in Druck). Die Enkelgeneration in der familialen Pflege bei Demenz: Erfahrungen und Bilanzierungen. Ergebnisse einer lebensweltorientierten Studie. [The grandchild generation in family care in dementia: experiences and balances. Results of a lifeworld-oriented study.] Zeitschrift für Gerontologie und Geriatrie, 44 (5).
Plemper, B. (2010). Ist Alzheimer eine Krankheit? [Is Alzheimer's disease a disease?] Psychologie heute, 5, 65-71.
Powell, J. (2009). Hilfen zur Kommunikation bei Demenz. [Communication aids for dementia.] Köln: Kuratorium Deutsche Altershilfe.
ProAlter (2011). Wer rastet, der rostet. Bewegungsangebote für Menschen mit Demenz. [A rolling stone gathers no moss. Movement offers for people with dementia.] ProAlter, 43 (2), 8.
Radzey, B. (2007). Angehörige: Spiritualität als Ressource der Entlastung? [Relatives: spirituality as a resource for relief?] DeSSorientiert, 2, 28-26. Stuttgart: Demenz Support Stuttgart. http://www.demenz-support.de /Repository/ dessjournal_2_2007_spiritualitaet.pdf [08.09.2011].
Rapp, M. A., Hellweg, R. & Heinz, A. (2011). Die Bedeutung depressiver Symptome bei beginnender Demenz vom Alzheimer-Typ im höheren Lebensalter. [The significance of depressive symptoms in incipient Alzheimer's disease-type dementia in older age.] Der Nervenarzt, 82 (9), 1140-1444
Rath, B. (2009). Eine grüne Idylle für Menschen mit Demenz. [A green idyll for people with dementia.] ProAlter, 1, 9-15.
Reith, W. & Essig, M. (2011). Neurodegenerative Erkrankungen und Demenz. [Neurodegenerative diseases and dementia.] Der Radiologe, 51 (4), 264-265.
Riedel, O., Dodel, R., Deuschl, G., Förstl, H., Heuser, I., Oertel, W., Reichmann, H., Riederer, P., Trenkwalder, C. & Wittchen, H. U. (2011). Demenz und Depression determinieren Pflegebedürftigkeit bei Morbus Parkinson: Untersuchung an 1449 Patienten im ambulanten Versorgungssektor in Deutschland. [Dementia and depression determine need for care in Parkinson's disease: study of 1449 patients in the ambulatory care sector in Germany.] Der Nervenarzt, 82 (8), 1012-1019.
Ruppert, N. (2011). Harn- und Stuhlinkontinenz bei Menschen mit einer Demenzerkrankung: „Wo war doch gleich die Toilette?“. [Urinary and fecal incontinence in people with dementia: "Where was the toilet again?".] Pflegezeitschrift, 64 (6), 334-337.
Oswald, W. D. (2004). Kognitive und körperliche Aktivität. Ein Weg zur Erhaltung von Selbstständigkeit und zur Verzögerung demenzieller Prozesse? [Cognitive and physical activity. A way to maintain independence and delay dementia processes?] Zeitschrift für Gerontopsychologie & -psychiatrie, 17 (3), 147-159.
Quarks & Co (2010). Alzheimer – Kampf gegen das Vergessen. [Alzheimer's disease - the fight against forgetting.] [TV magazine, 04/13/2010]. http://www.wdr.de/themen/global/webmedia/webtv/getwebtv.phtml?ref=70090 [01.07.2011].
Sachweh, S. (2009). Non-verbale Kommunikation. [Non-verbal communication.] DeSSorientiert, 1-2, 6-21. Stuttgart: Demenz Support Stuttgart. http://www.demenz-support.de/Repository/dessjournal_ 1_2_2009_hearing2.pdf [08.02.2024].
Saller, M. (2011). Innovative Bewegungsbetten helfen bei Schlafstörungen – Indikationsbezogene Varianten berücksichtigen individuelle Bedürfnisse. [Innovative motion beds help with sleep disorders - Indication-related variants take individual needs into account.] Pflegezeitschrift, 64 (4), 252.
Saß, H.; Wittchen, H.-U.; Zaudig, M. & Houben, I. (Hrsg.) (2003). Diagnostisches und Statistisches Manual Psychischer Störungen –Textrevision - DSM-IV-TR. [Diagnostic and statistical manual of mental disorders -Text revision - DSM-IV-TR.] Göttingen: Hogrefe.
Schabacher, C. (2011). Erleben im Hier und Jetzt. ADFC-Radtour mit Demenzerkrankten. [Experiencing in the here and now. ADFC cycling tour with dementia patients.] Radwelt. Das ADFC-Magazin, 4, 20-23.
Schmidt, R., Assem-Hilger, E., Benke, T., Dal-Bianco, P., Delazer, M. & Ladurner, G. (2008). Geschlechtsspezifische Unterschiede der Alzheimer Demenz. [Gender differences in Alzheimer's disease.] Neuropsychiatrie, 22 (1), 1–15
Schmidt, S. G., Palm, R., Dichter, M. & Hasselhorn, H. M. (2011). Arbeitsbedingte Prädiktoren für Zufriedenheit in der Demenzversorgung bei Pflegenden in stationären Altenpflegeeinrichtungen. [Work-related predictors of satisfaction in dementia care among caregivers in residential aged care facilities.] Pflege, 24 (2), 85-95.
Schmoeckel, M. (2010). Demenzerkrankungen als gesellschaftliche Herausforderung und Aufgabe für Juristen. [Dementia as a societal challenge and task for lawyers.] In M. Schmoeckel (Hrsg.), Demenz und Recht. Bestimmung der Geschäfts- und Testierfähigkeit. Baden-Baden: Nomos. 13-23.
Schönknecht, P., Sattler, C., Toro, P. & Essig, M. (2011). Klinik und bildgebende Diagnostik neurodegenerativer Demenzen. [Klinik und bildgebende Diagnostik neurodegenerativer Demenzen.] Der Radiologe, 51 (4), 278-284.
Schnell, M. W. & Mitzkat, A. (2006). „Demenz“ als Thema in der Literatur: Durch den Text zur Person. ["Dementia" as a topic in literature: through the text to the person.] Pflegezeitschrift, 1, 21-24.
Schnell, M. W. (2008). Fremdheit der Demenz – Grenze der Geisteswissenschaften. [Strangeness of dementia - frontier of the humanities.] In Tackenberg, P. & Abt-Zegelin, A. (Hrsg.), Demenz und Pflege. Eine interdisziplinäre Betrachtung. Frankfurt a.M.: Mabuse-Verlag. 77-82.
Schulte, S., Annicotte, I., Mowitz, A., Zerres, M., Braun, U., Joeres, U. & Jaehde, R. (2011). Pharmazeutische Betreuung eines Parkinson-Patienten mit orthostatischer Dysregulation. [Pharmaceutical management of a Parkinson's disease patient with orthostatic dysregulation.] Medizinische Monatsschrift für Pharmazeuten, 34 (7), 250-256.
Schulz, J. G. (2009). Seltene Ursachen. [Rare causes.] In R. Mahlberg & H. Gutzmann (Hrsg.), Demenzerkrankungen erkennen, behandeln und versorgen. Köln: Deutscher Ärzte-Verlag, 67-74.
Scottish Dementia Working Group (o.J.). About us. [Internetpräsenz]. http://www.sdwg. org.uk/home/about-us-sdwg/ [08.02.2024].
Scottish Government (2011). Promoting Excellence: A framework for all health and social services staff working with people with dementia, their families and carers. Edinburgh. http://www.scotland.gov.uk/Resource/Doc/350174/0117211.pdf [08.02.2024].
Shenk, D. (2005). Das Vergessen. Alzheimer: Portrait einer Epidemie. [The forgetting. Alzheimer's disease: portrait of an epidemic.] Leipzig: Europa-Verlag.
Staas, C. (2010). Je umstrittener, desto besser. Was taugen die Geschichtsartikel der Online-Enzyklopädie Wikipedia? Ein Gespräch mit dem Historiker Peter Haber. [The more controversial the better. What good are the history articles in the online encyclopedia Wikipedia? A conversation with historian Peter Haber.] Zeit Online, 10.07.2010. http://www.zeit.de/2010/28/Wikipedia-Daten [08.02.2024].
Stephan, I., Amthor, L. (2011). Tanzen im Sitzen: Lebensqualität und Gesundheitstraining: Singen, schwingen, schunkeln. [Dancing while sitting: Quality of life and health training: singing, swinging, swaying.] Pflegezeitschrift, 64 (6), 338-340.
Sterin, G. J. (2002). Essay on a word. A lived experience of Alzheimer’s disease. Dementia, 1, 7-10.
Strunk-Richter, G. & Krämer, A. (2008). Vom Schicksal der Sitzordnung. [About the fate of seating arrangements.] ProAlter, 4, 26-29.
Sust, C. (2009). Auswirkungen unterschiedlicher Beleuchtungen auf Demenzkranke. Erste Ergebnisse einer Studie. [Effects of different lighting on dementia patients. First results of a study.] ProAlter, 3, 27-32.
Suter, M. (1999). Small World. Zürich: Diogenes Verlag.
Taylor, R. (2008). Alzheimer und Ich. Leben mit Dr. Alzheimer im Kopf. [Alzheimer’s from the inside out.] Bern: Verlag Hans Huber. [Alzheimer's from the Inside Out, 2006]
Thomsen, M. (2011). „Man muss nicht jede Kuh vertreiben, die dem Demenzkranken begegnet.“ [Kommentar]. ["You don't have to drive away every cow the dementia patient encounters." Commentary]. Pflegezeitschrift, 64 (1), 12-13.
Voigt-Radloff, S. & Hüll. M. (2011). Alltagsbewältigung bei Demenz: Medikamentöse und nicht medikamentöse Interventionen zeigen kleine Effekte auf heterogenen Skalen. [Coping with daily life in dementia: Medication and non-medication interventions show small effects on heterogeneous scales.] Psychiatrische Praxis 38 (5), 221-231.
Wahl, H.-W. & Heyl, V. (2004). Gerontologie – Einführung und Geschichte. [Gerontology - Introduction and History]. Stuttgart: Kohlhammer.
Wallesch, C. W. (2011). Alzheimer-Krankheit und senile Demenz. Editorial. [Alzheimer's Disease and Senile Dementia. Editorial]. Fortschritte der Neurologie – Psychiatrie, 79 (3), 137.
Weber, S (2005). Kommen nach den "science wars" die "reference wars"? Wandel der Wissenskultur durch Netzplagiate und das Google-Wikipedia-Monopol. [Are the "reference wars" coming after the "science wars"? Changes in the culture of knowledge through network plagiarism and the Google Wikipedia monopoly.] Telepolis [Online-Magazin] vom 29.09.2005. http://www.heise.de/tp/artikel/20/20982/1.html [08.02.2024]
Weinreich, W. M. (2005). Integrale Psychotherapie. Ein umfassendes Therapiemodell auf der Grundlage der Integralen Philosophie nach Ken Wilber. [Integral Psychotherapy. A comprehensive therapy model based on the Integral Philosophy according to Ken Wilber]. Leipzig: Araki-Verlag.
Weinreich, W. M. (2007). Integrale Psychotherapie. [Integral Psychotherapy] http://integrale-psychotherapie.de/Resources/Integrale_Psychotherapie_R_ Artikel.pdf [01.09.2011].
Werner, S. (2011). Bewegung bei Menschen mit Demenz. Autonomie respektieren. [Movement in People with dementia. Respecting autonomy.] Pflegezeitschrift, 64 (4), 205-206.
Werner, S. (in Druck). Demenz: Reflexionen zur Sterbebegleitung. „Der Tod berührt ihn nicht im Kern. [Dementia: reflections on end-of-life care. "Death does not touch him at his core.”] Pflegezeitschrift, 64 (9), 528-531.
Wetzstein, V. (2005a). Diagnose Alzheimer. Grundlagen einer Ethik der Demenz. Frankfurt a.M.: Campus Verlag.
Wetzstein, V. (2005b). Alzheimer-Demenz. Perspektiven einer integrativen Demenz-Ethik. [Diagnosis of Alzheimer's disease. Foundations of an ethics of dementia.] Zeitschrift für medizinische Ethik, 51, 27-40.
Wetzstein, V. (2006). Alzheimer-Demenz: Entstehung eines Krankheitsbegriffs. [Alzheimer's disease: emergence of a concept of disease.] In Nationaler Ethikrat (Hrsg.), Altersdemenz und Morbus Alzheimer. Medizinische, gesellschaftliche und ethische Herausforderungen. Vorträge der Jahrestagung des Nationalen Ethikrates 2005. (37-48). Berlin: Nationaler Ethikrat.
World Health Organization [WHO] (2007): Meeting of the International Advisory Group for the Revision of ICD-10 Mental and Behavioural Disorders 24 – 25 September 2007, Geneva, Switzerland. http://www.who.int/mental_health/evidence/icd_summary _report_sept_2007.pdf [24.06.2011].
Whitehouse, P.J. & George, D. (2009). Mythos Alzheimer. Was Sie schon immer über Alzheimer wissen wollten, Ihnen aber nicht gesagt wurde. [The Myth of Alzheimer's: What You Aren't Being Told About Today's Most Dreaded Diagnosis]. Bern: Verlag Hans Huber.
Wikipedia. Diskussion: Integrale Theorie. [Version vom 25.09.2011]. http://de.wikipedia.org /wiki/Diskussion:Integrale_Theorie.
Wikipedia. Entität. [Version vom 18.08.2011]. http://de.wikipedia.org/wiki/Entität.
Wikipedia. Ethnomethodologie. [Version vom 31.05.2011]. http://de.wikipedia.org/wiki/Ethnomethodologie.
Wikipedia. Holon. [Version vom 20.08.2011]. http://de.wikipedia.org/wiki/Holon.
Wikipedia. Integrale Theorie. [Version vom 25.09.2011]. http://de.wikipedia.org/wiki/Integrale_Theorie
Wikipedia. Integral Theory. [Version vom 25.09.2011]. http://en.wikipedia.org/wiki/Integral _Theory
Wikipedia. Konzept. [Version vom 27.09.2011]. http://de.wikipedia.org/wiki/Konzept
Wikipedia. Noumenon. [Version vom 18.08.2011]. http://de.wikipedia.org/wiki/Noumenon
Wikipedia. Phänomen. [Version vom 18.08.2011]. http://de.wikipedia.org/wiki/Phänomen
Wikipedia. Talk:Integral Theory. [Version vom 25.09.2011]. http://en.wikipedia.org/wiki/Talk:Integral_Theory
Wikipedia. Wikipedia:Enzyklopädie/Qualitätssicherung in der Wikipedia. [Version vom 01.10.2011]. http://de.wikipedia.org/wiki/Wikipedia:Enzyklopädie/Qualitätssicherung_in _der_Wikipedia
Wikipedia. Wikipedia. [Version vom 02.10.2011]. http://de.wikipedia.org/wiki/Wikipedia
Wilber, K. (1997). The Eye of the Spirit. An Integral Vision for a World Gone Slightly Mad. [German: Das Wahre, Schöne, Gute. Geist und Kultur im 3. Jahrtausend (2005). Frankfurt a.M.: Fischer Taschenbuch Verlag, 2. Auflage.]
Wilber, K. (1996). A brief history of everything. [German: Eine kurze Geschichte des Kosmos. (1999) Frankfurt a.M.: Fischer Taschenbuch Verlag, 3. Auflage.]
Wilber, K. (2000a). Sex, Ecology, Spirituality. [German: Eros, Kosmos, Logos. Eine Jahrtausend-Vison (2006a). Frankfurt a.M.: Fischer Taschenbuch-Verlag, 4. Auflage.]
Wilber, K. (2000b). Integral Psychology: Consciousness, Spirit, Psychology, Therapy [German: Integrale Psychologie. Geist – Bewusstsein – Psychologie – Therapie. (2001b) Freiamt: Arbor-Verlag]
Wilber, K. (2001a). Ganzheitlich handeln. Eine integrale Vision für Wirtschaft, Politik, Wissenschaft und Spiritualität. [A Theory of Everything. An Integral Vidion for Business, Politis, Science and Spirituality.] Freiamt: Arbor-Verlag.
Wilber, K. (2006a). Integral Spirituality. A Startling New Role for Religion in the Modern and Postmodern World. [German: Integrale Spiritualität. Spirituelle Intelligenz rettet die Welt (2007). Kösel-Verlag: München.]
Wilber, K. (2006b). Excerpt B: The Many Way We Touch. Three Principles Helpful for Any Integrative Approach. http://www.kenwilber.com/writings/read_pdf/84 [22.09.2010].
Wilber, K. (2006c). Excerpt A: An Leading Age at the Leading Age. http://www.kenwilber.com/writings/read_pdf/83 [22.09.2011].
Wilber, K. (2007). The Integral Vision. A Very Short Introduction to the Revolutionary Integral Approach to Life, God, the Universe, and Everything. [German: Integrale Vision. Eine kurze Geschichte der integralen Spiritualität. (2009) München: Kösel-Verlag.]
Wingenfeld, K, Seidl, N. & Ammann, A. (2011). Präventive Unterstützung von Heimbewohnern mit Verhaltensauffälligkeiten. [Preventive support for nursing home residents with behavioral problems.] Zeitschrift für Gerontologie & Geriatrie, 44 (1), 27-32.
Wißmann, P. & Gronemeyer, R. (2008). Demenz und Zivilgesellschaft – eine Streitschrift. [Dementia and civil society - a polemic]. Frankfurt a.M.: Mabuse-Verlag.
Wittrock, D. (2008). Perspektiven inter- und transdisziplinärer Kooperation im Lichte des integralen methodologischen Pluralismus Ken Wilbers. Masterarbeit [Perspectives on inter- and transdisciplinary cooperation in the light of Ken Wilber's integral methodological pluralism. Master‘s thesis]. Bremen. http://integralesleben.org/fileadmin/user_upload/LESESAAL/PDF/Transdisziplinaritaet_und_IMP_DW.pdf [27.08.2011].
Wolter, D. K. (2009). Risiken von Antipsychotika im Alter, speziell bei Demenzen. Eine Übersicht. [Risks of antipsychotics in old age, especially in dementia. A survey.] Zeitschrift für Gerontopsychologie & -psychiatrie, 22 (1), 17–5.
Ziegler, U. & Doblhammer, G. (2009). Prävalenz und Inzidenz von Demenz in Deutschland. Eine Studie auf Basis von Daten der gesetzlichen Krankenversicherungen von 2002. [Prevalence and incidence of dementia in Germany. A study based on 2002 statutory health insurance data.] Gesundheitswesen, 71, 281 – 290
Zimmermann, C. (2009). „Es gibt ein Leben nach der Diagnose!“. Interview mit P. Wissmann. ["There is a life after diagnosis!". Interview with P. Wissmann.] Pflegen: Demenz, 1, 6-9.